- New stuff to read and discuss
- What patients say
- Clinic / online appointments
- Why the diagnosis of a psychosomatic illness is often a misdiagnosis
- Vascular Compression Syndromes
- Do you have questions?
- Checklist vascular compression syndromes
- Description of your symptoms
- Researchers from the Mayo Clinic confirm my concept of the Midline Congestion Syndrome
- Explanation of gender-specific differences in the clinical symptoms of abdominal vascular compression syndromes: varicocele and penile/testicular pain – their main manifestation in men.
- Varicocoele is predominantly caused by left renal vein compression
- Musculoskeletal pecularities of female puberty
- Lordosis /Swayback- Origin of many abdominal compression syndromes
- Bending of a straight vein compels its narrowing
- The lordogenetic midline congestion syndrome
- Neurological consequences of the midline congestion syndrome
- Successful treatment of a teenage girl who was unable to eat due to extreme postprandial pain and unable to walk due to spasticity in her left leg
- Severe ataxia in a young woman with severe spinal congestion – complete resolution after decompression of the left renal vein
- All compression syndromes are one: the spectrum of lordogenetic compressions
- Nutcracker-Syndrome is a misnomer! Lordogenetic left renal vein compression is a more appropriate name!
- May-Thurner-constellation (May-Thurner-syndrome, Cockett’s syndrome)
- Midline (congestion) syndrome
- Pelvic congestion syndrome
- Celiac Trunk Compression / Dunbar syndrome / MALS / Arcuate ligament syndrome
- Wilkie-Syndrome / Superior-mesenteric-artery-syndrome
- Compression of the vena cava inferior
- Evlauation of vascular compressions with the PixelFlux-method
- Connective tissue disorders predispose to multiple compressions
- Postural tachycardia syndrome (POTS) – the hemodynamic consequence of vascular compression syndromes and loose connective tissue
- Restless legs-a little known symptom of abdominal vascular compression syndromes
- Pudendal neuralgia in vascular compression syndromes
- A new sonographic sign of severe orthostatic venous pooling
- Migraine and Multiple Sclerosis
- Hemodynamic effect on cerebral perfusion in patients with multiple localised vascular compression.
- Treatment of vascular compression syndromes
- Fatal errors in the treatment of vascular compression syndromes
- Risks of stents in venous compression syndromes
- Surgical treatment of abdominal compression syndromes: The significance of hypermobility‐related disorders
- Nutcracker and May-Thurner syndrome: Decompression by extra venous tube grafting and significance of hypermobility related disorders
- Our surgical treatment of vascular compressions
- Chronic regional pain syndrome (CRPS) caused by venous compression and mechanical irritation of the coeliac plexus
- Vascular compression syndromes and other disease mechanisms I recently detected
- Kaleidoscope of instructive cases
- Venous congestion of the spinal cord may be a potential contributor to the development of paraplegia in patients with spinal muscular atrophy type III (Kugelberg-Welander disease)
- Ultrasound Diagnostics
- A breakthrough in functional sonographic diagnostic – 4D-colour Doppler sonographic flow volume measurements
- 4D-volume flow measurements of jugular and mesenteric veins
- Inauguration of the global volumetric brain perfusion measurement-a gateway for understanding of neurological symptoms
- Ultrasound focused entirely on all of your symptoms
- Ultrasound vs. X-ray
- Vascular Malformations
- Profile
- Functional colour Doppler ultrasound – how I do it
- Perfusion Measurement – PixelFlux-method
- Research
- Publications
- Nutcracker and May-Thurner syndrome: Decompression by extra venous tube grafting and significance of hypermobility related disorders
- Papers authored by Th. Scholbach
- Publications
- Inauguration of measurements of the tissue pulsatility index in renal transplants
- From nutcracker phenomenon to midline congestion syndrome and its treatment with aspirin
- First sonographic tissue perfusion measurement in renal transplants
- First sonographic bowel wall perfusion measurement in Crohn disease
- First sonographic renal tissue perfuison measurement
- First sonographic measurement of renal perfusion loss in diabetes mellitus
- PixelFlux measurements of renal tissue perfusion
- Why I prefer not to publish in journals but in the Internet
- Vessel stretching in nephroptosis – an important driver of complaints
- Publications
- Expertise
- Bornavirus Infection
- Scientific cooperation
- Cookie Policy
- Data protection
- Cookie Policy (EU)
- Impressum
Menstrual pain – not an irrevocable fate but a reversible consequence of vascular compression syndromes
Well over 90% of all patients with vascular compression syndromes are girls and women. So, you could talk about a typical woman’s disease here. The reason for this is the anatomical peculiarities in the structure of the pelvic skeleton in women.
During puberty, the pelvis of girls grows more strongly than the pelvis of boys’ in width and depth. Both growth processes favor the development of a particularly pronounced lordosis (hollow back).
By widening the pelvis, the lumbar muscles, which pull from the lumbar spine to the inner thigh and function to flex the hip joint and pull the thigh inward, exert a stronger traction on the lumbar spine of women. Since the spine cannot be compressed, this muscle traction causes a forward curvature of the lumbar spine and thus increased lordosis.
The greater depth of the pelvis in women exerts a greater leverage effect on the hip joint because the hip joint is not in the center of the hip but behind the central line. As a result, the pelvis tilts forward and downwards. This too, produces a stronger lordosis of the lumbar spine, since the lumbar spine attaches directly to the sacrum, which is firmly connected to the other hip bones.
The increased curvature of the lumbar spine in women, depending on the extent of the lordosis, sometimes has serious effects on their internal organs. The left renal vein, which runs in front of the spine will become compressed at the vertex of the lordosis. The blood of the congested left renal vein the runs downwards, via the left ovarian vein, into the pelvis.
The second most common feature in the development of compression syndromes is the compression of the nervous plexus around the celiac trunk, exerted by the traction of the diaphragmatic crura, which are attached to the lumbar spine. This disease is called arcuate ligamentum syndrome or Dunbar syndrome.
Later, the tilting of the pelvis often causes the sacrum to be pressed against the left common iliac vein from behind. Consequently, this vein is compressed between the sacral bone and the right common iliac artery. This disease is called May-Thurner-Syndrome.
Initially, often during puberty, typical symptoms of women are mainly upper abdominal pain (due to left renal vein compression and celiac plexus irritation) and the commonly considered “normal” menstrual cramps.
From the aspect of vascular compression syndromes, severe menstrual pain is readily understandable.
Much of the blood which is trapped wihtin the renal vein and left common iliac vein must pass across the uterus and ovaries to reach the inferior vena cava on the right side of the spine. It must move from the left to right side of the body. Other organs, also located in the midline of the pelvis, such as the bladder, rectum, and vagina, are often affected too since they become bridges for the congested blood.
Only if the blood from the left hemisphere of the pelvis passes easily, merely unresisted, through the uterus, than the pressure within the left pelvic or spinal veins is so little that the women are not in pain.
During the menstrual cycle, however, blood flow through the uterus changes considerably. At the beginning of the cycle the lining of the uterus builds up and the blood flow gradually increases.
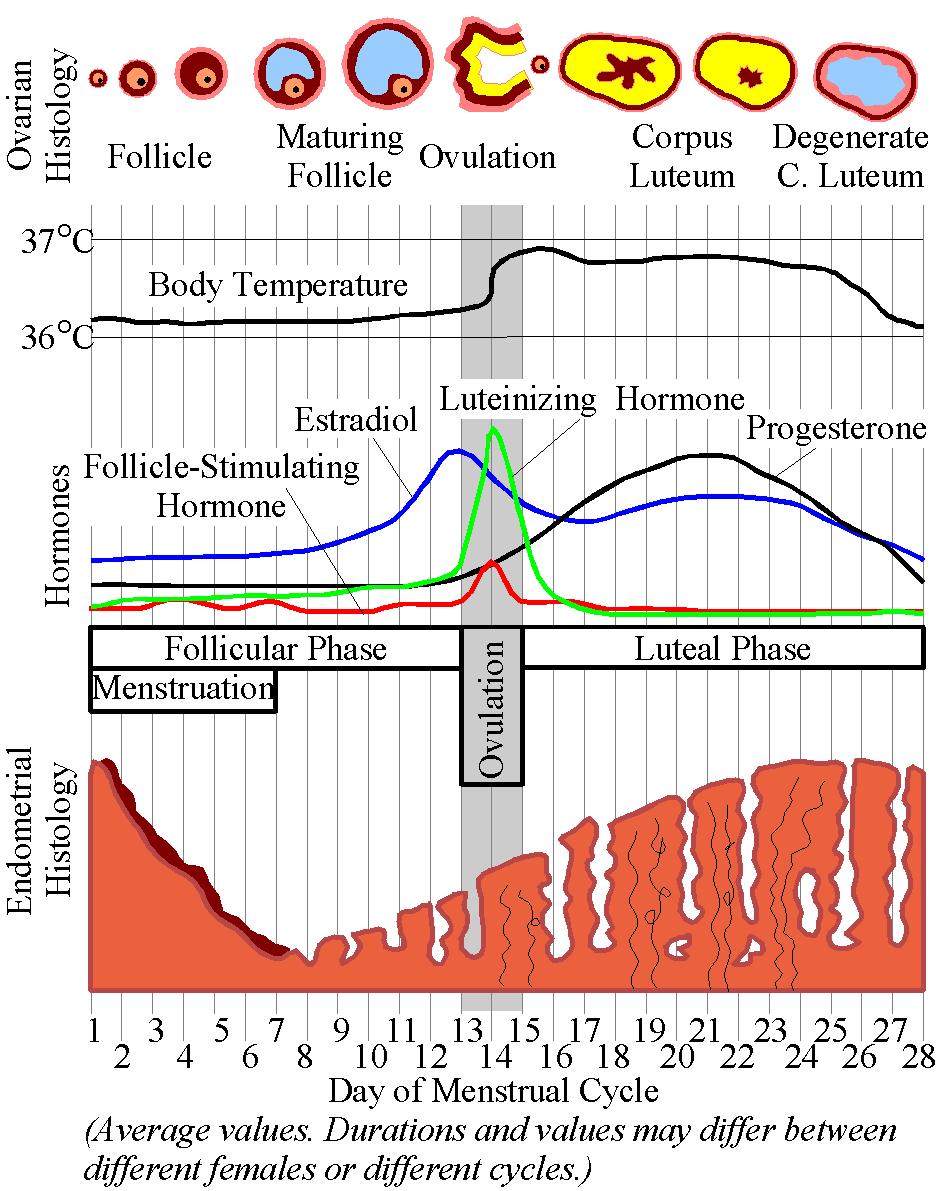
from: https://upload.wikimedia.org/wikipedia/commons/f/f0/MenstrualCycle.png
With ovulation, around the 14th day of the cycle, once again a rapid increase in circulation is observed. This allows a much better transit of blood through the uterus. However, shortly before the onset of menstrual bleeding, the blood flow to the uterus drops sharply. This has been scientifically demonstrated in both magnetic resonance imaging and transvaginal Doppler sonography.

from: In Vivo Perfusion, T 1, and T 2 Measurements in the Female Pelvis During the Normal Menstrual Cycle: A Feasibility Study Caroline L. Hoad, PhD, Jonathan Fulford, PhD, Nick J. Raine-Fenning, PhD, Bruce K. Campbell, PhD, Ian R. Johnson, PhD, and Penelope A. Gowland, PhD in: JOURNAL OF MAGNETIC RESONANCE IMAGING 24: 1350-1356 (2006)
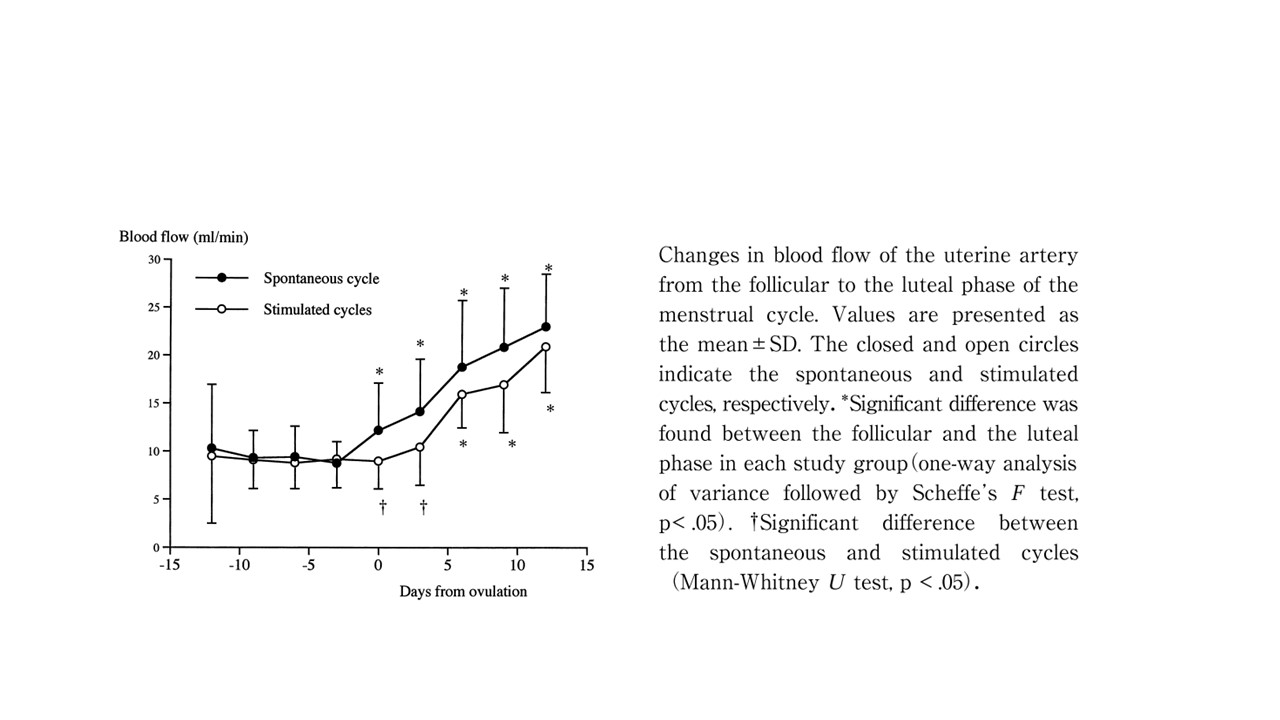
from: Assessment of Endometrial Perfusion with Doppler Ultrasound in Spontaneous and Stimulated Menstrual Cycles Akihito Nakai, Akishige Yokota, Tatsuo Koshino and Tsutomu Araki in: J Nippon Med Sch 2002; 69 (4)
Suddenly, a high resistance against the transit of blood, which is pooled within the left pelvic hemisphere, develops. Accordingly, the pressure in the left uterine, ovarian and pelvic veins increases steeply. Since these veins are inflamed as a result of their chronic distension, the fast pressure rise within the left pelvic veins leads to severe menstrual pain.