- Neue Artikel
- Was Patienten sagen – Fortsetzung
- Praxis/ online Terminvergabe
- Warum die Diagnose einer psychosomatischen Erkrankung häufig eine Fehldiagnose ist
- Gefäßkompressionssyndrome
- Haben Sie Fragen?
- Checkliste Gefäßkompressionssyndrome
- Beschreibung Ihrer Symptome
- Erklärung der geschlechtsspezifischen Unterschiede bei den klinischen Symptomen von abdominalen vaskulären Kompressionssyndromen: Varikozele und Penis-/Hodenschmerzen – ihre Hauptmanifestation bei Männern.
- Die Varikozele wird überwiegend durch eine Kompression der linken Nierenvene verursacht
- Muskuloskelettale Besonderheiten der weiblichen Pubertät
- Lordose /Hohlkreuz – Ursache zahlreicher abdomineller Kompressionssyndrome
- Die Anhebung einer Vene erzwingt deren Kompression
- Truncuskompression bei Kindern
- Lordogenetisches Mittellinensyndrom
- Neurologische Folgen des Mittellinienstauungssyndroms
- Erfolgreiche Behandlung einer Teenagerin, die aufgrund extremer postprandialer Schmerzen nicht essen und aufgrund einer Spastik im linken Bein nicht gehen konnte.
- Schwere Ataxie bei einer jungen Frau mit schwerer venöser Rückenmarksstauung – vollständige Heilung nach Dekompression der linken Nierenvene
- Alle abdominalen Kompressionssyndrome liegen in der Lordose begründet
- Das „Nussknacker“-Syndrom ist eine Fehlbezeichnung
- May-Thurner-Konstellation /May-Thurner-Syndrom/Cockett’s syndrome/Vena iliaca-Kompressionssyndrom
- Mittelliniensyndrom (Stauung der Mittellinienorgane)
- Pelvines Kongestionssyndrom
- Truncus-coeliacus-Kompression / Dunbar-Syndrom / MALS / Ligamentum arcuatum-Syndrom
- Wilkie-Syndrom / Arteria-mesenterica-superior-Syndrom
- Kompression der Vena cava inferior
- Quantifizierung der Gefäßkompressionssyndrome mit der PixelFlux-Technik
- Bindegewebserkrankungen begünstigen kombinierte Kompressionssyndrome
- Posturales Tachykardiesyndrom (POTS) – die hämodynamische Folge von Gefäßkompressionssyndromen und lockerem Bindegewebe
- Unruhige Beine (restless legs) – Folge venöser Kompressionssyndrome
- Pudendusneuralgie bei vaskulären Kompressionssyndromen
- Ein neues sonographisches Zeichen für eine schwere orthostatische Beckenvenenstauung
- Migräne und Multiple Sklerose
- Behandlung von Kompressionssyndromen
- Fehler bei der Therapie von Gefäßkompressionssyndromen
- Embolisation – Irrweg bei venösen Kompressionssyndromen
- Risiken von Stents bei venösen Kompressionssyndromen
- Chirurgische Behandlung von abdominalen Kompressionssyndromen: Die Bedeutung der Bindegewebshypermobilität
- Nutcracker and May-Thurner syndrome: Decompression by extra venous tube grafting and significance of hypermobility related disorders
- Chronisches regionales Schmerzsyndrom (CRPS) verursacht durch Venenkompressionen und mechanische Reizung des Plexus coeliacus
- Vaskuläre Kompressionssyndrome, die ich kürzlich entdeckt habe
- Kaleidoskop lehrreicher Krankheitsverläufe
- Eine venöse Stauung im Rückenmark kann möglicherweise zur Entwicklung einer Querschnittslähmung bei Patienten mit spinaler Muskelatrophie beitragen.
- Ultraschalldiagnostik
- Leistungsspektrum
- Funktioneller Farbdoppler-Ultraschall – wie ich ihn verstehe
- Durchblutungsmessung – PixelFlux-Verfahren
- Forschung
- Publikationen
- Nutcracker and May-Thurner syndrome: Decompression by extra venous tube grafting and significance of hypermobility related disorders
- Veröffentlichungen von Th. Scholbach
- Eigene Publikationen
- Erstbeschreibung der Bestimmung des Gewebsperfusionsindexes in Nierentranplantaten
- Erstbeschreibung des Mittellininesyndroms – Aspirintherapie
- Erste sonografische Gewebsperfusionsmessung in Nierentransplantaten
- Erste sonografische Tumorperfusionmessung und Korrelation zur Tumoroxygenierung
- Erstmalige Darmwandperfusionsmessung bei M. Crohn
- Erstmalige sonografische Gewebsperfusionmessung der Nieren
- Erstmaliger Nachweis von Frühveränderungen der Nierenperfusion bei Diabetes mellitus
- PixelFluxmessung der Nierengewebsperfusion
- Publikationen
- Expertise
- Bornavirusinfektion
- Wissenschaftliche Zusammenarbeit
- Cookie-Richtlinie
- Hinweise zu medizinischen Erläuterungen
- Datenschutzerklärung
- Cookie Policy (EU)
- Impressum
Schwere Ataxie bei einer jungen Frau mit ausgeprägter venöser Rückenmarksstauung – vollständige Heilung nach Dekompression der linken Nierenvene
Es gibt zahlreiche Folgen einer Stauung des Rückenmarks als Folge der Kompression der linken Nierenvene und der linken Beckenvene bei Patienten mit Mittellinienstauungssyndrom.
Die möglichen zahlreichen klinischen Folgen werden auf einer separaten Seite beschrieben.
Ich berichte hier über eine junge Frau, die auf der Grundlage eines hypermobilen Ehlers-Danlos-Syndroms multiple abdominale Kompressionssyndrome mit zunehmender Ataxie (Balancestörung des Rumpfes und des Kopfes), schwere vegetative Symptome, starke Bauchschmerzen, Krämpfe und gynäkologische Probleme entwickelte.
Aufgrund der progredienten Ataxie des Rumpfes, des Kopfes und der Extremitäten musste sie sich eines Rollstuhls bedienen. Die neurologische Routinediagnostik und bildgebende Standardverfahren in ihrem Heimatland und im Ausland führten nicht zu einem behandelbaren Grund für ihr Leiden.
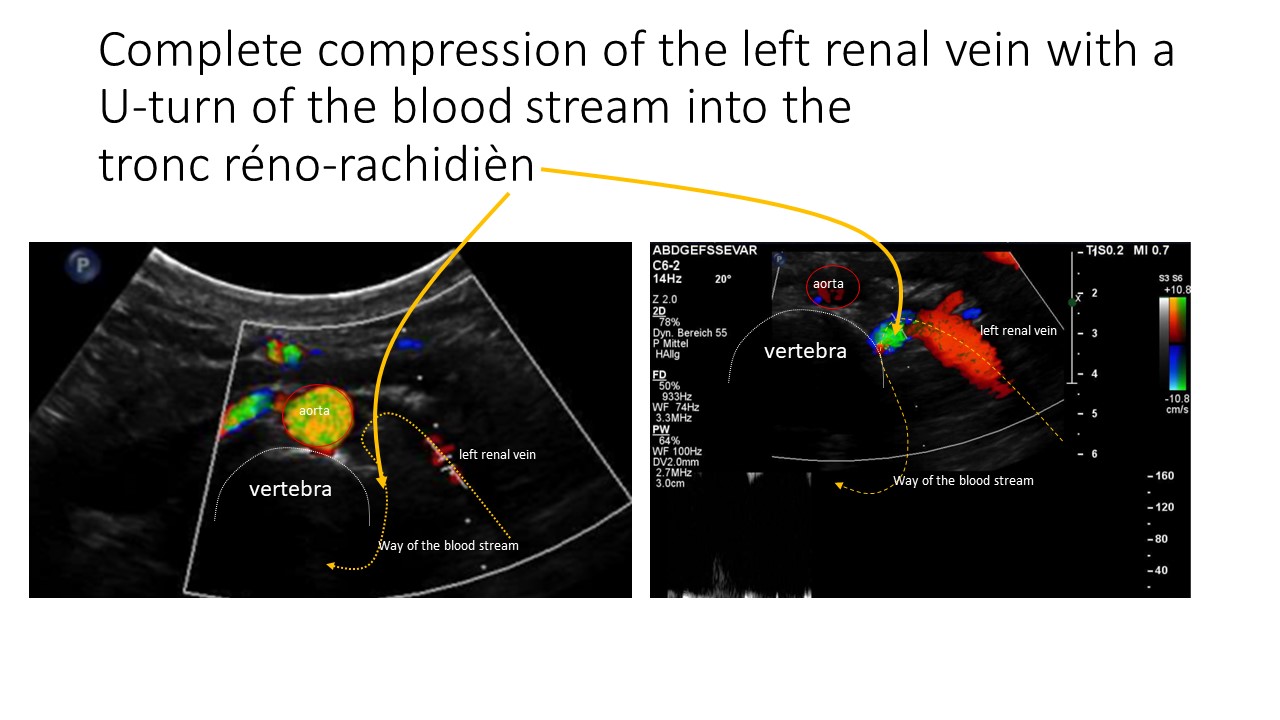
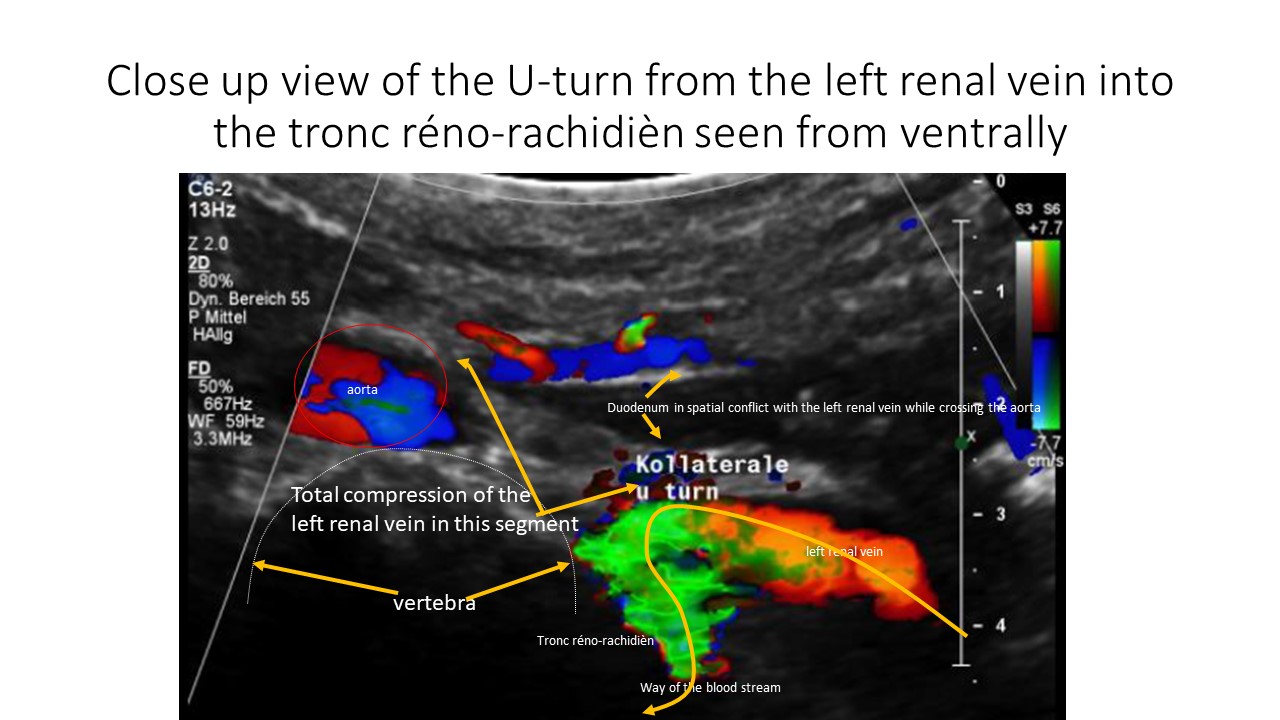
Erst die funktionelle Farbdopplersonographie mit Quantifizierung aller relevanten Bauch- und Beckengefäße konnte die eigentliche Ursache ihres Leidens aufzeigen – eine massive venöse Stauung des Rückenmarks, gespeist durch einen stark durchbluteten Tronc réno-rachidièn. Dieses Gefäß verband die gestaute und vollständig verschlossene linke Nierenvene mit dem epiduralen Venenplexus im Wirbelkanal. Dadurch entwickelte sich eine schwere venöse Stauung des Rückenmarks. Dies führte zu Krämpfen und einer Instabilität des Rumpfes und Kopfes.
Dieses Video zeigt ihren erbarmungswürdigen Zustand vor der Operation im Mai 2022
Das folgende Video wurde im März 2023 aufgenommen, 7,5 Monate nach der erfolgreichen Dekompression der linken Nierenvene und dem anschließenden vollständigen Versiegen des Tronc réno-rachidièn
Krankengeschichte
Januar 2016
Übererregbarkeit, Muskelkrämpfe, Gewichtszunahme aufgrund von Ödemen in den Beinen
Januar 2017
Wurde wegen schwerer Muskelkrämpfe und Anfälle in die Notaufnahme eingeliefert
Herzrhythmusstörungen, Schwindel, Erbrechen, Taubheitsgefühl in beiden Händen und Zittern des Rumpfes
Sucht mehrmals die Notaufnahme des psychiatrischen Krankenhauses wegen allgemeiner Zittrigkeit auf. Dort wurde bei ihr eine psychische Störung diagnostiziert: Angststörung
Februar 2017
Vorstellung in der Notaufnahme mit Schmerzen auf der rechten Seite der Wirbelsäule und häufigem Harndrang bei Entleerung kleiner Urinportionen (Pollakisurie)
Einweisung in die psychiatrische Abteilung wegen wiederholter generalisierter Krämpfe
Psychiater lehnt die Diagnose einer Angststörung ab
Mai 2017
Es wurde ein Syndrom der bakteriellen Darmüberwucherung und eine eosinophile Ösophagitis diagnostiziert
Mai 2021
War bei vielen Ärzten im Heimatland und im Ausland, ohne eine angemessene Diagnose und Behandlung für ihre zunehmende Rumpfinstabilität und die Krämpfe zu erhalten
Sie leidet auch an Unterleibsschmerzen, die unter dem Zwerchfell lokalisiert sind und nach beiden Seiten ausstrahlen und nach dem Essen (postprandial) zunehmen
Sie kann nicht richtig atmen
Schwierigkeiten beim Schlucken
Schmerzen in der Brust
ist ständig aufgeregt
Starke Benommenheit, Sehstörungen, Migräne, Schwindel, Gefühl, betrunken zu sein, Rückenschmerzen, kalte und bläuliche Hände, schwache Füße und Hände
Zunehmende Müdigkeit und schnelle Erschöpfbarkeit
Überstreckbarkeit (Hyperflexibilität) der Gelenke
Erstmalige Vorstellung in meiner Sprechstunde für funktionelle Farbdoppler-Sonographie im Juni 2021
Bei der ersten Untersuchung wurden folgende Diagnosen gestellt:
- Beckenvenenstauungssyndrom (Pelvic Congestion Syndrome) als Folge von
- May-Thurner-Syndrom mit venösem Sporn
- Schwere Lendenlordose als Hauptursache für alle vaskulären Kompressionssyndrome der Patientin
- Komplette lordogenetische Kompression der linken Nierenvene mit einem Bypass über einen
- Tronc réno-rachidièn, der sich in den Plexus epiduralis ergießt und damit das Rückenmark venös staut, und eine
- erweiterte linke Ovarialvene, die das Blut in Richtung Becken ableitet
- Erhebliche zusätzliche venöse Stauung der Beckenvenen in aufrechter Körperhaltung als Zeichen einer klinisch relevanten Bindegewebsstörung – in Übereinstimmung mit bestimmten klinischen Zeichen einer solchen Störung: hypermobiles Ehlers-Danlos-Syndrom
- Schweres Ligamentum arcuatum-Syndrom (Dunbar Syndrom)
- Absinken beider Nieren im Stehen (orthostatische Ptose)
- Starke orthostatische Drosselung des Blutflusses in Richtung beider Nieren, vor allem auf der linken Seite aufgrund der Nierenptose bei aufrechter Körperhaltung – dies trägt wesentlich zur
- Ansammlung von venösem Blut im Becken und in beiden Beinen bei
- Starke Verringerung des zirkulierenden Blutvolumens in der Aorta bei aufrechter Körperhaltung
- Doppelte Gebärmutter




Präoperative Messung der Perfusion des Nierenparenchyms im Juni 2021
![]()
Die Patientin wurde im Juni 2021 und im Juli 2022 operiert, wobei eine Dekompression des Truncus coeliacus durchgeführt und die linke Vena iliaca communis und die linke Nierenvene mit einem ringverstärkten PTFE-Transplantat vom Druck der kreuzenden Arterien abgeschirmt wurden.
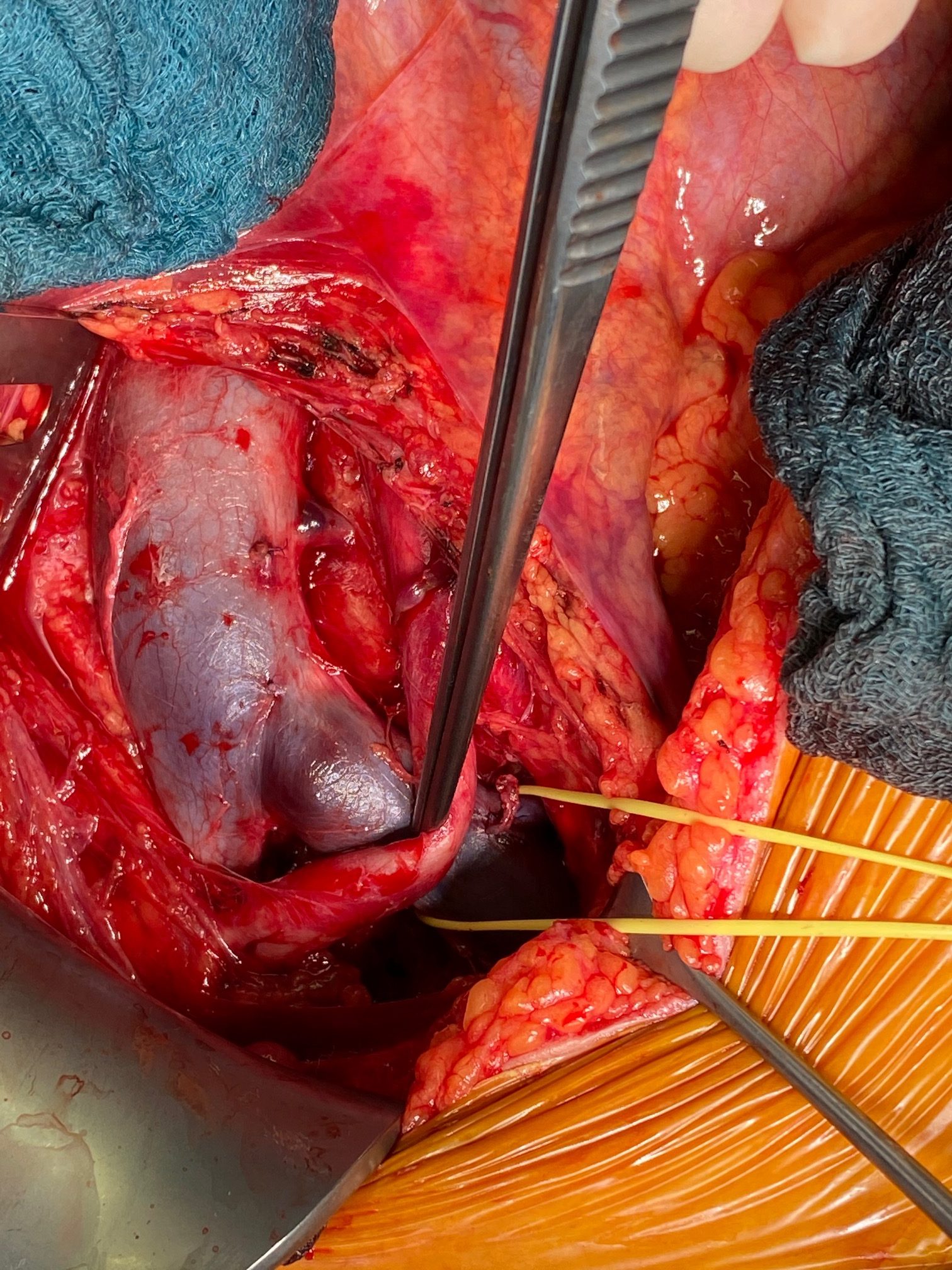
Die Operation wurde von Professor Sandmann in der Klinik BelEtage in Düsseldorf (Deutschland) durchgeführt. Ich bin ihm sehr dankbar für seine aufgeschlossene Kooperation und die Erlaubnis, seine intraoperativen Fotos zu veröffentlichen.

Befreiung des Truncus coeliacus nach Durchtrennung von massivem Narbengewebe, das ihn komprimiert hatte

Schwere Kompression der linken Beckenhauptvene durch die kreuzende rechte Beckenarterie – sonographisch diagnostiziertes May-Thurner-Syndrom
Degenerierte Wand der linken Vena iliaca communis an der Kreuzungsstelle mit der rechten Arteria iliaca communis

Freigelegte linke Nierenvene mit dem Tronc réno-rachidièn (gelb angeschlungen – rot: Vena ovarica, blau: Vena suprarenalis)
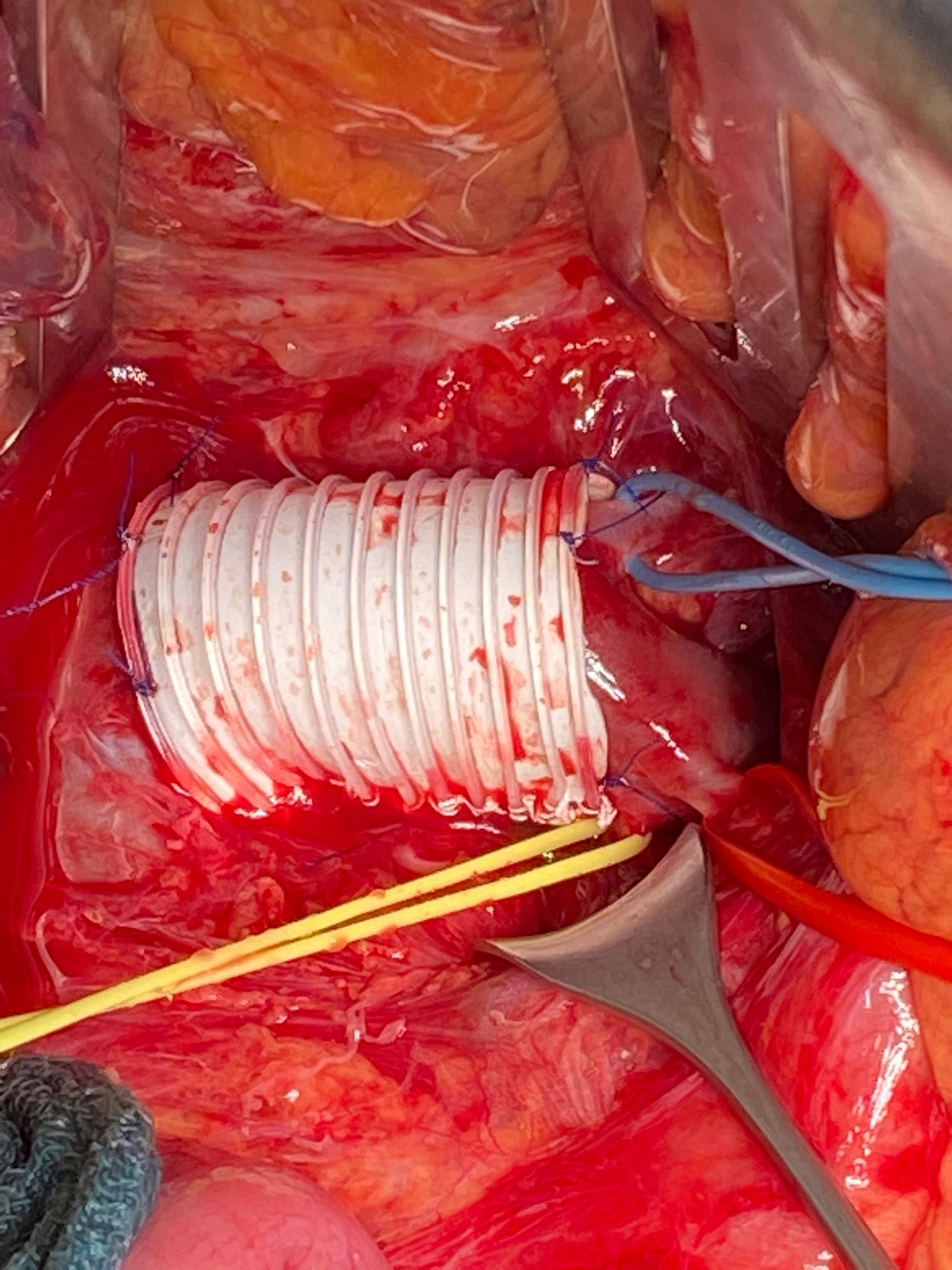
PTFE-Schild um die linke Nierenvene, um sie vor der Kompression durch die Aorta zu schützen
Postoperative Nierenparenchym-Durchblutungsmessung im November 2022 nach zusätzlicher Dekompression der linken Nierenvene durch ein PTFE-Schild im Juli 2022
![]()
In aufrechter Haltung betrug das Verhältnis von linker zu rechter Nierendurchblutung präoperativ bei 12 % und liegt nun bei 31 %.
Insgesamt wurde durch die Operation eine wesentlich bessere Durchblutung der linken Niere erreicht, indem das Flussvolumen der linken Niere um 87 % gesteigert werden konnte.
Gleichzeitig war kein Blutfluss mehr über den Tronc réno-rachidièn nachweisbar, während präoperativ etwa 1000 mL/min über den Tronc réno-rachidièn in den Plexus epiduralis gepresst wurden. Dies führte zu einem erheblichen Druckanstieg des Hirnwassers mit venöser Rückenmarksstauung.
Die Wiedereröffnung der linken Nierenvene durch Umhüllung mit einer PTFE-Hülse führte zum Versiegen des Blutstroms über den Tronc réno-rachidièn. Das klinische Ergebnis ist ein vollständiges Verschwinden aller neurologischen Symptome der Patientin!
Wir (Prof. Sandmann und ich) danken der Patientin für ihre Genehmigung diesen Bericht und ihre Videos zu veröffentlichen und vor allem für ihre Standhaftigkeit, bei einem in ihrer Heimat nicht zu klärenden, fortschreitenden, schweren Krankheitsbild die Hoffnung auf Heilung nicht aufgegeben zu haben!