- New stuff to read and discuss
- What patients say
- Clinic / online appointments
- Why the diagnosis of a psychosomatic illness is often a misdiagnosis
- Vascular Compression Syndromes
- Do you have questions?
- Checklist vascular compression syndromes
- Description of your symptoms
- Researchers from the Mayo Clinic confirm my concept of the Midline Congestion Syndrome
- Explanation of gender-specific differences in the clinical symptoms of abdominal vascular compression syndromes: varicocele and penile/testicular pain – their main manifestation in men.
- Varicocoele is predominantly caused by left renal vein compression
- Musculoskeletal pecularities of female puberty
- Lordosis /Swayback- Origin of many abdominal compression syndromes
- Bending of a straight vein compels its narrowing
- The lordogenetic midline congestion syndrome
- Neurological consequences of the midline congestion syndrome
- Successful treatment of a teenage girl who was unable to eat due to extreme postprandial pain and unable to walk due to spasticity in her left leg
- Severe ataxia in a young woman with severe spinal congestion – complete resolution after decompression of the left renal vein
- All compression syndromes are one: the spectrum of lordogenetic compressions
- Nutcracker-Syndrome is a misnomer! Lordogenetic left renal vein compression is a more appropriate name!
- May-Thurner-constellation (May-Thurner-syndrome, Cockett’s syndrome)
- Midline (congestion) syndrome
- Pelvic congestion syndrome
- Celiac Trunk Compression / Dunbar syndrome / MALS / Arcuate ligament syndrome
- Wilkie-Syndrome / Superior-mesenteric-artery-syndrome
- Compression of the vena cava inferior
- Evlauation of vascular compressions with the PixelFlux-method
- Connective tissue disorders predispose to multiple compressions
- Postural tachycardia syndrome (POTS) – the hemodynamic consequence of vascular compression syndromes and loose connective tissue
- Restless legs-a little known symptom of abdominal vascular compression syndromes
- Pudendal neuralgia in vascular compression syndromes
- A new sonographic sign of severe orthostatic venous pooling
- Migraine and Multiple Sclerosis
- Hemodynamic effect on cerebral perfusion in patients with multiple localised vascular compression.
- Treatment of vascular compression syndromes
- Fatal errors in the treatment of vascular compression syndromes
- Risks of stents in venous compression syndromes
- Surgical treatment of abdominal compression syndromes: The significance of hypermobility‐related disorders
- Nutcracker and May-Thurner syndrome: Decompression by extra venous tube grafting and significance of hypermobility related disorders
- Our surgical treatment of vascular compressions
- Chronic regional pain syndrome (CRPS) caused by venous compression and mechanical irritation of the coeliac plexus
- Vascular compression syndromes and other disease mechanisms I recently detected
- Kaleidoscope of instructive cases
- Venous congestion of the spinal cord may be a potential contributor to the development of paraplegia in patients with spinal muscular atrophy type III (Kugelberg-Welander disease)
- Ultrasound Diagnostics
- A breakthrough in functional sonographic diagnostic – 4D-colour Doppler sonographic flow volume measurements
- 4D-volume flow measurements of jugular and mesenteric veins
- Inauguration of the global volumetric brain perfusion measurement-a gateway for understanding of neurological symptoms
- Ultrasound focused entirely on all of your symptoms
- Ultrasound vs. X-ray
- Vascular Malformations
- Profile
- Functional colour Doppler ultrasound – how I do it
- Perfusion Measurement – PixelFlux-method
- Research
- Publications
- Nutcracker and May-Thurner syndrome: Decompression by extra venous tube grafting and significance of hypermobility related disorders
- Papers authored by Th. Scholbach
- Publications
- Inauguration of measurements of the tissue pulsatility index in renal transplants
- From nutcracker phenomenon to midline congestion syndrome and its treatment with aspirin
- First sonographic tissue perfusion measurement in renal transplants
- First sonographic bowel wall perfusion measurement in Crohn disease
- First sonographic renal tissue perfuison measurement
- First sonographic measurement of renal perfusion loss in diabetes mellitus
- PixelFlux measurements of renal tissue perfusion
- Why I prefer not to publish in journals but in the Internet
- Vessel stretching in nephroptosis – an important driver of complaints
- Publications
- Expertise
- Bornavirus Infection
- Scientific cooperation
- Cookie Policy
- Data protection
- Cookie Policy (EU)
- Impressum
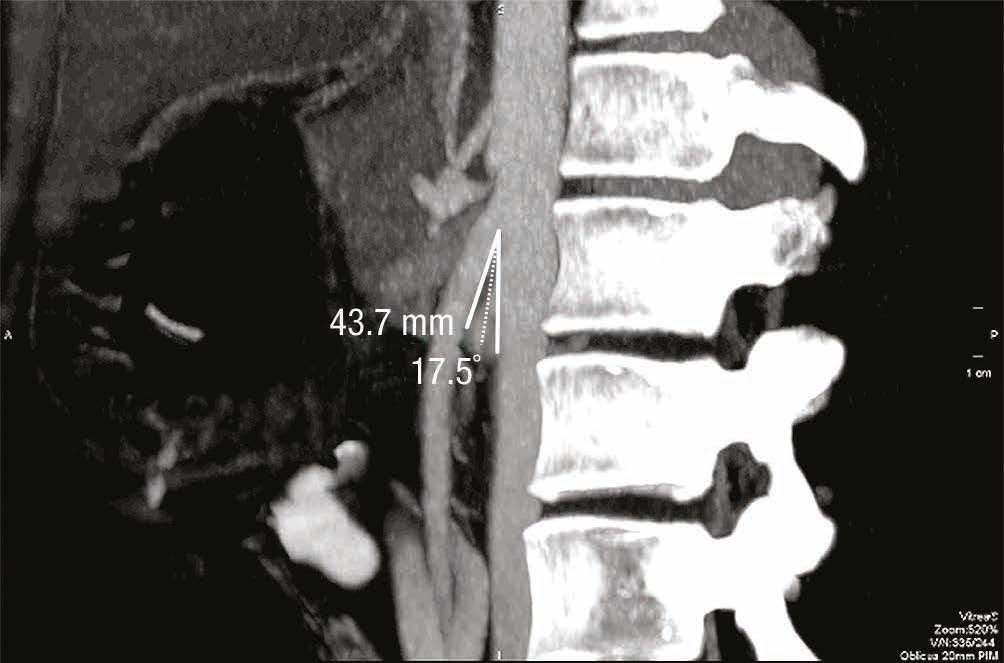
The problem of angle measurement in Wilkie syndrome
Compression of the duodenum between the aorta and the superior mesenteric artery can result in a obstruction of the passage in the horizontal duodenal segment with severe postprandial upper abdominal pain, vomiting, belching, nausea and can then lead to considerable weight loss. This clinical picture is referred to as superior mesenteric artery syndrome, SMA syndrome or Wilkie syndrome.
To diagnose this clinical picture, functional sonography is required during and after food intake, which shows that the food runs against the clamp of the aorta and superior mesenteric artery and the right-sided portion of the horizontal portion of the duodenum expands considerably, while the portion between the two arteries remains narrow. In typical cases, this should result in a configuration similar to that of a curved clamp.

Compression of the duodenum at high peristaltic pressure and even higher counterpressure of the vascular clamp from the aorta (bottom) and superior mesenteric artery (top)
This makes it clear that a strong driving force is pushing the duodenum against the clamp of the aorta and superior mesenteric artery, so that the duodenum is maximally dilated and yet is unable to widen the gap between the aorta and superior mesenteric artery sufficiently to ensure adequate transportation of food.
The diagnosis is often made when the angle between the aorta and the superior mesenteric artery is narrow.
In my many years of personal experience with many patients presenting with a suspected diagnosis of Wilkie syndrome, I must advise against relying on this angle sign.
For several reasons, this sign is completely unreliable:
- Firstly, the angle between the two vessels may widen during the passage of food, as the duodenum normally exerts sufficient force to lift the superior mesenteric artery. Since the angle between the two arteries is often measured on an empty stomach, it is easy to see that a narrow aorto-mesenteric angle cannot be a reliable criterion in a fasting patient, since in everyday life the problems do not occur on an empty stomach but on a full stomach. A CT scan after food intake can also be misleading, as the duodenum only contracts at longer intervals. If the image was taken between two contraction waves, the angle between the two arteries can collapse again and therefore simulate a narrowing that disappears when the duodenum contracts.The only reliable method here is functional sonography, i.e. continuous observation of the horizontal duodenal segment and the other parts of the duodenum after ingestion, in which the patient plays an important role. The patient must describe which symptoms occur or do not occur as soon as the food passes between the aorta and the superior mesenteric artery. This passage is followed on the screen together with the patient. This is not possible in CT or MRI anyway, as the patient is alone in the room. Only from the combination of subjective symptoms described by the patient and the simultaneous stop
At best, similar statements can be made with fluoroscopy after food intake. In this case, however, the arteries cannot be seen directly, the intestine is clearly visible as it is filled with high-contrast “food” (barium swallow). However, it can be shown whether there is a blockage in the right-sided portion of the horizontal duodenal segment. However, the examination is associated with radiation exposure, whereas the ultrasound examination is completely harmless and can use the food that causes the patient particular difficulties in real life.
- With the angle method, it should also be noted that when viewing the angle from the side (angle measurement in the sagittal plane), a narrow angle can also appear if the arteries diverge laterally. In this case, a narrow angle when viewed from the side results in a wide angle when viewed from above (frontal plane). However, often only the angle in the sagittal plane is determined. However, the duodenum can snake under the laterally deviated superior mesenteric artery and snake over the aorta without being constricted at any point.
{kind=link}
Angle measurements are therefore unsuitable for detecting Wilkie syndrome.