- New stuff to read and discuss
- What patients say
- Clinic / online appointments
- Why the diagnosis of a psychosomatic illness is often a misdiagnosis
- Vascular Compression Syndromes
- Do you have questions?
- Checklist vascular compression syndromes
- Description of your symptoms
- Researchers from the Mayo Clinic confirm my concept of the Midline Congestion Syndrome
- Explanation of gender-specific differences in the clinical symptoms of abdominal vascular compression syndromes: varicocele and penile/testicular pain – their main manifestation in men.
- Varicocoele is predominantly caused by left renal vein compression
- Musculoskeletal pecularities of female puberty
- Lordosis /Swayback- Origin of many abdominal compression syndromes
- Bending of a straight vein compels its narrowing
- The lordogenetic midline congestion syndrome
- Neurological consequences of the midline congestion syndrome
- Successful treatment of a teenage girl who was unable to eat due to extreme postprandial pain and unable to walk due to spasticity in her left leg
- Severe ataxia in a young woman with severe spinal congestion – complete resolution after decompression of the left renal vein
- All compression syndromes are one: the spectrum of lordogenetic compressions
- Nutcracker-Syndrome is a misnomer! Lordogenetic left renal vein compression is a more appropriate name!
- May-Thurner-constellation (May-Thurner-syndrome, Cockett’s syndrome)
- Midline (congestion) syndrome
- Pelvic congestion syndrome
- Celiac Trunk Compression / Dunbar syndrome / MALS / Arcuate ligament syndrome
- Wilkie-Syndrome / Superior-mesenteric-artery-syndrome
- Compression of the vena cava inferior
- Evlauation of vascular compressions with the PixelFlux-method
- Connective tissue disorders predispose to multiple compressions
- Postural tachycardia syndrome (POTS) – the hemodynamic consequence of vascular compression syndromes and loose connective tissue
- Restless legs-a little known symptom of abdominal vascular compression syndromes
- Pudendal neuralgia in vascular compression syndromes
- A new sonographic sign of severe orthostatic venous pooling
- Migraine and Multiple Sclerosis
- Hemodynamic effect on cerebral perfusion in patients with multiple localised vascular compression.
- Treatment of vascular compression syndromes
- Fatal errors in the treatment of vascular compression syndromes
- Risks of stents in venous compression syndromes
- Surgical treatment of abdominal compression syndromes: The significance of hypermobility‐related disorders
- Nutcracker and May-Thurner syndrome: Decompression by extra venous tube grafting and significance of hypermobility related disorders
- Our surgical treatment of vascular compressions
- Chronic regional pain syndrome (CRPS) caused by venous compression and mechanical irritation of the coeliac plexus
- Vascular compression syndromes and other disease mechanisms I recently detected
- Kaleidoscope of instructive cases
- Venous congestion of the spinal cord may be a potential contributor to the development of paraplegia in patients with spinal muscular atrophy type III (Kugelberg-Welander disease)
- Ultrasound Diagnostics
- A breakthrough in functional sonographic diagnostic – 4D-colour Doppler sonographic flow volume measurements
- 4D-volume flow measurements of jugular and mesenteric veins
- Inauguration of the global volumetric brain perfusion measurement-a gateway for understanding of neurological symptoms
- Ultrasound focused entirely on all of your symptoms
- Ultrasound vs. X-ray
- Vascular Malformations
- Profile
- Functional colour Doppler ultrasound – how I do it
- Perfusion Measurement – PixelFlux-method
- Research
- Publications
- Nutcracker and May-Thurner syndrome: Decompression by extra venous tube grafting and significance of hypermobility related disorders
- Papers authored by Th. Scholbach
- Publications
- Inauguration of measurements of the tissue pulsatility index in renal transplants
- From nutcracker phenomenon to midline congestion syndrome and its treatment with aspirin
- First sonographic tissue perfusion measurement in renal transplants
- First sonographic bowel wall perfusion measurement in Crohn disease
- First sonographic renal tissue perfuison measurement
- First sonographic measurement of renal perfusion loss in diabetes mellitus
- PixelFlux measurements of renal tissue perfusion
- Why I prefer not to publish in journals but in the Internet
- Vessel stretching in nephroptosis – an important driver of complaints
- Publications
- Expertise
- Bornavirus Infection
- Scientific cooperation
- Cookie Policy
- Data protection
- Cookie Policy (EU)
- Impressum
Lordosis /hollow back : cause of numerous abdominal compression syndromes.
Physiology of lordosis in humans and other bipeds
Pathogenic consequences of an increased lordosis
Necessity of a functional sonographic diagnostics of lordosis
Lordosis is the forward curvature of a segment of the spine.
Physiology of lordosis in humans and other bipeds
The upright gait of humans represents a special feature among animal modes of locomotion. With the onset of learning to walk, from about the 11th month of life, it changes the shape of the spine from a simple arch of the recumbent infant to the double-Pelt-S-shaped form of the upright walking adult.
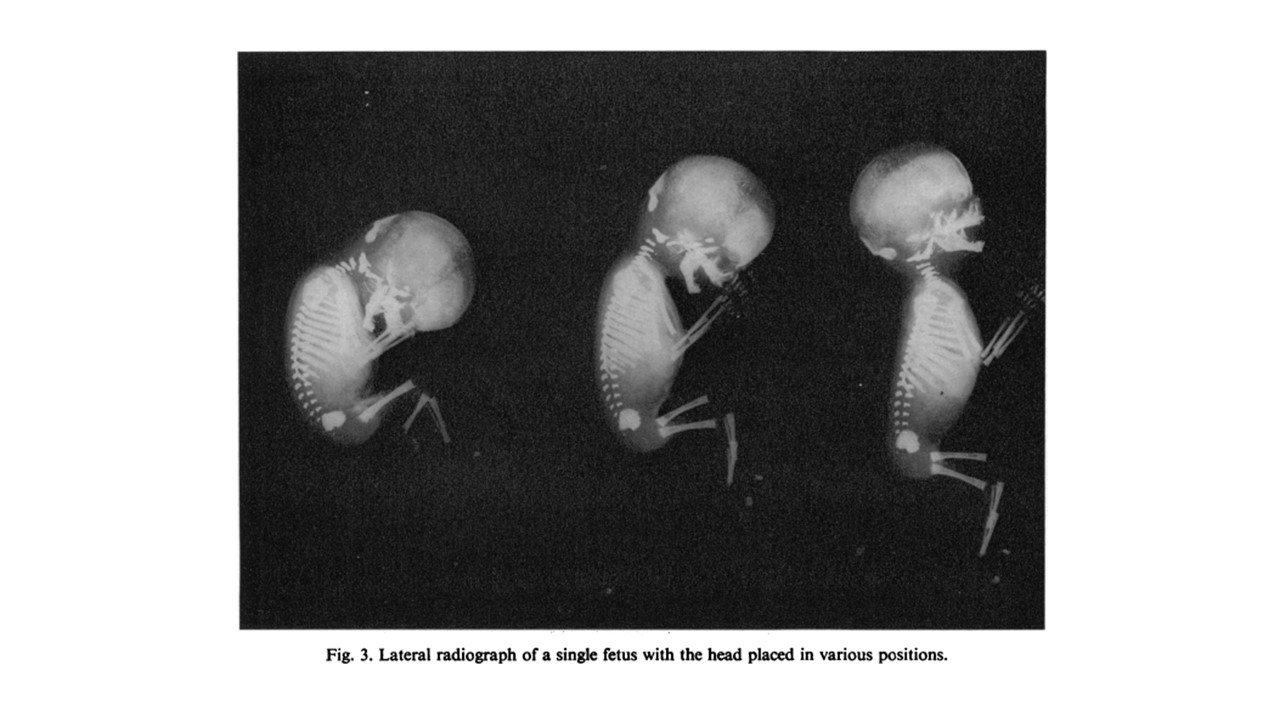
The spine of the human fetus is C-shaped (left picture). In the crawling child, a lordosis of the cervical spine develops , the lumbar lordosis is not yet established – right picture). Fig. from:K. M. BAGNALL, P. F. HARRIS AND P. R. M. JONES. A radiographic study of the human fetal spine. 1. The development of the secondary cervical curvature. J. Anat. (1977), 123, 3, pp. 777-782

The adult spine shows the distinct lumbar lordosis (LL), as well as thoracic kyphosis (TK) which develop with the bipedal gait of humans after 1 year of age. Copyright © 2013 Hasan Ghandhari et al. Fig off.: BioMed Research International, Volume 2013 (2013), Article ID 842624, 7 pages http://dx.doi.org/10.1155/2013/842624, Assessment of Normal Sagittal Alignment of the Spine and Pelvis in Children and Adolescents Hasan Ghandhari, Hamid Hesarikia, Ebrahim Ameri, and Abolfazl Noori
In other bipeds (certain species of dinosaurs and the birds and kangaroos that evolved from them), the thoracic and lumbar spines run horizontally, so gravity does not affect the longitudinal axis of the spine.
In humans, on the other hand, the direction of gravity and the longitudinal axis of the spine are in the same plane. Therefore, the flexible spine collapses. The ligaments of the spine determine with their individual extensibility how far the individual vertebrae can shear forward or backward from the perpendicular gravitational axis. They have to shear out because the entire spine is exposed not only to the perpendicularly acting gravity but also to forces that deviate from the direction of gravity – the forces of locomotion, bending and lateral inclination – our voluntary motor activity.
In addition, the human hip joint is structured like that of a quadruped and therefore has its natural resting point at about 90 ° of hip flexion. In an upright posture, the joint must therefore be maximally extended, often hyperextended, and in addition the pelvis is tilted forward to compensate for the anatomical inability of the joint to be further extended when standing. The forced pelvic tilt forward can now only be compensated for by a compensatory curvature of the lumbar spine backward – this is lordosis. Work by my father, the orthopedic surgeon Dr. Manfred Scholbach, has revealed these mechanical peculiarities of the human pelvis, which until then had been misinterpreted as an extensor inhibition of the infant hip. The infant’s hip is already fully extended when he or she is kicking while lying on his or her back with “flexed” hip joints and cannot bring the thigh into contact with the support. Whoever, as an adult, sleeps lying on his back with stretched legs or “stretches” his hip joints while standing, is therefore overstretching his hip joints and, in addition, forcing the lordosis that is considered normal in humans.
Pathogenic consequences of increased lordosis
This lordosis assumes a different degree in individual people. It is co-determined by numerous factors.
The extent of lordosis is described by Euler’s laws, Euler case 2).
Lordosis is aggravated by high body length, soft connective tissue (the spinal ligaments consist of connective tissue), flabby muscles, weak musculature (especially the gluteal muscles), spinal anomalies, expansive body masses in the chest and abdominal region (overweight people, pregnant women and women with heavy breasts), pelvic tilting forward. Females are generally affected by more lordosis than males because of more pelvic tilt and than pre-pubertal girls. During puberty, the pelvis grows more forward in girls – this tends to cause the front edge of the pelvis to drop. It also grows more to either side. This leads to a stronger pull of the hip flexor muscles (psoas muscles) on the lumbar spine. These muscles connect the lumbar vertebrae to the inner edge of the femur. If the distance between the femurs gradually widens in girls during puberty, there tends to be a downward pull on the lumbar spine. Since the vertebrae cannot be compressed (it is only osteoporosis in older women that causes the lumbar vertebrae to sinter together), the spine can only follow the downward pull by curving more sharply – lordosis increases.
Women are therefore particularly affected by all secondary diseases of increased lordosis. These sequelae include vascular compression of the abdomen, thigh and knee, to the pull of the diaphragm on the solar plexus and compression of the intestine between vessels (aorta and superior iliac artery) or between the aorta and the abdominal wall.
The individual clinical pictures are shown here: Truncus and ganglion coeliacum compression, nutcracker syndrome, Wilkie syndrome, vena cava compression syndrome, femoral vein compression, popliteal vein compression, May-Thurner syndrome, pelvic congestion, compression of renal arteries and spinal arteries by the diaphragm.
Necessity of sonographic functional diagnostics of lordosis
Lordosis can often be detected on physical examination. In many cases, however, the sonographically determined degree of lordosis is surprising. Sometimes, at the apex of the lordotic spinal curvature, only a few millimeters of distance to the internal abdominal wall border remain and the extent of compression of internal organs is not visible to the affected person from the outside.
Therefore, it is essential to accurately visualize the lordosis and the compressed structures in dynamic ultrasound. The compressed vessels and organs are examined sonographically in various body postures. The pressure in the vessels is determined with color Doppler ultrasound, and the impairment of organ function is measured with PixelFlux software.
The first goal in the treatment of these compression disorders, before any medication or surgical treatment measures that may be necessary later, is therefore to reduce the lordosis. Physiotherapy, special sports and yoga exercises can be used for this purpose. Then, suitable exercises, footwear and seating furniture as well as bed constructions are recommended to reduce lordosis and compression.
Please refer to our notes on medical explanations on this website.