- Neue Artikel
- Was Patienten sagen – Fortsetzung
- Praxis/ online Terminvergabe
- Warum die Diagnose einer psychosomatischen Erkrankung häufig eine Fehldiagnose ist
- Gefäßkompressionssyndrome
- Haben Sie Fragen?
- Checkliste Gefäßkompressionssyndrome
- Beschreibung Ihrer Symptome
- Erklärung der geschlechtsspezifischen Unterschiede bei den klinischen Symptomen von abdominalen vaskulären Kompressionssyndromen: Varikozele und Penis-/Hodenschmerzen – ihre Hauptmanifestation bei Männern.
- Die Varikozele wird überwiegend durch eine Kompression der linken Nierenvene verursacht
- Muskuloskelettale Besonderheiten der weiblichen Pubertät
- Lordose /Hohlkreuz – Ursache zahlreicher abdomineller Kompressionssyndrome
- Die Anhebung einer Vene erzwingt deren Kompression
- Truncuskompression bei Kindern
- Lordogenetisches Mittellinensyndrom
- Neurologische Folgen des Mittellinienstauungssyndroms
- Erfolgreiche Behandlung einer Teenagerin, die aufgrund extremer postprandialer Schmerzen nicht essen und aufgrund einer Spastik im linken Bein nicht gehen konnte.
- Schwere Ataxie bei einer jungen Frau mit schwerer venöser Rückenmarksstauung – vollständige Heilung nach Dekompression der linken Nierenvene
- Alle abdominalen Kompressionssyndrome liegen in der Lordose begründet
- Das „Nussknacker“-Syndrom ist eine Fehlbezeichnung
- May-Thurner-Konstellation /May-Thurner-Syndrom/Cockett’s syndrome/Vena iliaca-Kompressionssyndrom
- Mittelliniensyndrom (Stauung der Mittellinienorgane)
- Pelvines Kongestionssyndrom
- Truncus-coeliacus-Kompression / Dunbar-Syndrom / MALS / Ligamentum arcuatum-Syndrom
- Wilkie-Syndrom / Arteria-mesenterica-superior-Syndrom
- Kompression der Vena cava inferior
- Quantifizierung der Gefäßkompressionssyndrome mit der PixelFlux-Technik
- Bindegewebserkrankungen begünstigen kombinierte Kompressionssyndrome
- Posturales Tachykardiesyndrom (POTS) – die hämodynamische Folge von Gefäßkompressionssyndromen und lockerem Bindegewebe
- Unruhige Beine (restless legs) – Folge venöser Kompressionssyndrome
- Pudendusneuralgie bei vaskulären Kompressionssyndromen
- Ein neues sonographisches Zeichen für eine schwere orthostatische Beckenvenenstauung
- Migräne und Multiple Sklerose
- Behandlung von Kompressionssyndromen
- Fehler bei der Therapie von Gefäßkompressionssyndromen
- Embolisation – Irrweg bei venösen Kompressionssyndromen
- Risiken von Stents bei venösen Kompressionssyndromen
- Chirurgische Behandlung von abdominalen Kompressionssyndromen: Die Bedeutung der Bindegewebshypermobilität
- Nutcracker and May-Thurner syndrome: Decompression by extra venous tube grafting and significance of hypermobility related disorders
- Chronisches regionales Schmerzsyndrom (CRPS) verursacht durch Venenkompressionen und mechanische Reizung des Plexus coeliacus
- Vaskuläre Kompressionssyndrome, die ich kürzlich entdeckt habe
- Kaleidoskop lehrreicher Krankheitsverläufe
- Eine venöse Stauung im Rückenmark kann möglicherweise zur Entwicklung einer Querschnittslähmung bei Patienten mit spinaler Muskelatrophie beitragen.
- Ultraschalldiagnostik
- Leistungsspektrum
- Funktioneller Farbdoppler-Ultraschall – wie ich ihn verstehe
- Durchblutungsmessung – PixelFlux-Verfahren
- Forschung
- Publikationen
- Nutcracker and May-Thurner syndrome: Decompression by extra venous tube grafting and significance of hypermobility related disorders
- Veröffentlichungen von Th. Scholbach
- Eigene Publikationen
- Erstbeschreibung der Bestimmung des Gewebsperfusionsindexes in Nierentranplantaten
- Erstbeschreibung des Mittellininesyndroms – Aspirintherapie
- Erste sonografische Gewebsperfusionsmessung in Nierentransplantaten
- Erste sonografische Tumorperfusionmessung und Korrelation zur Tumoroxygenierung
- Erstmalige Darmwandperfusionsmessung bei M. Crohn
- Erstmalige sonografische Gewebsperfusionmessung der Nieren
- Erstmaliger Nachweis von Frühveränderungen der Nierenperfusion bei Diabetes mellitus
- PixelFluxmessung der Nierengewebsperfusion
- Publikationen
- Expertise
- Bornavirusinfektion
- Wissenschaftliche Zusammenarbeit
- Cookie-Richtlinie
- Hinweise zu medizinischen Erläuterungen
- Datenschutzerklärung
- Cookie Policy (EU)
- Impressum
Kompression der Vena cava inferior
Compression of the vena cava inferior by/against the lumbar spine and the diaphragm
During the workup of patient with the compression syndromes a compression of the vena cava inferior or is frequently found in combination with other compression syndromes-mainly May Thurner syndrome and lordogenetic left renal vein compression aka nutcracker syndrome.
The review of the medical literature does not retrieve any scientific papers describing the situation.
Thus, I am going to report my own experiences with compression of the vena cava in different body and breathing postures.
A compression can only be exerted by neighbouring structures. So, the vena cava can be compressed by the spine with its vertebra and intervertebral discs, the small and large bowel, the liver, the diaphragm, the right common iliac artery and the right renal artery. Within the thorax the pericardium, the pleura and lung structures may compress the vena cava.
Beside these normal anatomic structures tumors, abscessi and malformations due to their variable location may compress the vena cava. Such conditions are not taken into consideration in the following description.
The right kidney lies too far dorsally to compress the vena cava, especially if the lordotic curvature of the spine is exaggerated, the pancreas lies left to the vena cava stretching across the midline to the left, and the abdominal wall usually does not the vena cava in contrary to the aorta since the vena cava lies at the right circumference of the vertebrae and their lateral processi whereas the aorta usually lies only slightly left to the midline and more prominent at the ventral surface of the vertebra thus being the first structure of the retroperitoneum been touched by the abdominal wall is an increased lordosis is pushing the retroperitoneal structures ventrally.
Compression of the vena cava inferior by the spine
The vena cava is frequently compressed running along the lordotic curvature of the lumbar spine if this curvature is exaggerated. This can best be evaluated not by x-ray but ultrasound or MRI or CT. The hallmark of an exaggerated lordosis in the context of vascular compression syndromes is a substantial narrowing of the abdominal cavity in front of the lumbar spine.
In patients with a relevant compression of the vena cava inferior the minimum distance from the ventral surface of the spine or the frequently protruding intervertebral disc (mostly L2/L3 or L3/L4) at the apex of the lordotic curvature towards the inner lining of the abdominal wall is often less than 2 cm. Not rarely it may undercut 1 cm!
In these patients the vena cava is quite frequently compressed at typical locations. The numbers also indicate the frequency of the occurrence of the compression:
- Immediately cranial to the mouth of the left common iliac vein
- Exactly at the apex of the lordotic curvature
- At the cranial slope of the lordotic curvature while standing only
- At the cranial slope of the lordotic curvature while lying supine after a meal due to the enlargement of a dysfunctional descending portion of the duodenum
- By the diaphragm within the caval opening of the diaphragm
While the first compression sites are usually found in a supine posture-the patient is lying on his/her back-the compression at the cranial slope of the lordotic curvature can usually be only found while the trunk is an upright position-standing or sitting.
The symptoms may encompass the symptoms of the nutcracker syndrome and the may Thurner syndrome plus localized pain at the compression site.
Thus, main symptoms are usually :
- Discoloration of the feet and legs
- Swelling of the legs
- Leg pain
- Pain in the pelvis (mainly the genitals and around the anus)
- Urinary bladder dysfunction
- Left flank pain and mid abdominal pain
- Sharp and stabbing pain underneath the 8th to 10th rib on the right side especially while standing
- Dull pain under the right lower rib cage – a sharp, stabbing pain here in situations where the venous return is increased and therefore the pressure in the vena cava: Physical activity, bending forward, standing upright (if there are other compressions, especially of the left renal vein and the left common iliac vein).
- Swelling of the liver
- Disturbed digestion
- Sensation of fullness in the upper abdomen mainly on the right side
The diagnosis is straightforward with a functional colour Doppler sonographic ultrasound examination and is most precise while using the PixelFlux technique. The most important obstacle for a correct diagnosis of a vena cava compression is not taking it into consideration.
The following images demonstrate typical findings in patients with vena cava inferior compression
- Respiration-dependent collapse of the vena cava inferior at the height of the lordotic curvature

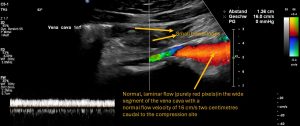
- Constant significant narrowing of the vena cava inferior in comparison to uncompressed segment of the vein


locally circumscribed compression of the vena cava by a protruding intervertebral disc as a consequence of the increased bulging of the spine

elongated compression the vena cava inferior by the spine
- Typical circumscribed flow acceleration of the vena cava inferior at the compression site

- Typically localized turbulences highlighted by green and yellow colored pixels inside the vena cava inferior
- Compression of the vena cava while standing by the downsinking liver squeezing the vena cava against the cranial slope of the lordotic curvature of the spine
- While standing

- Disappearance of the compression while lying horizontally

- While standing
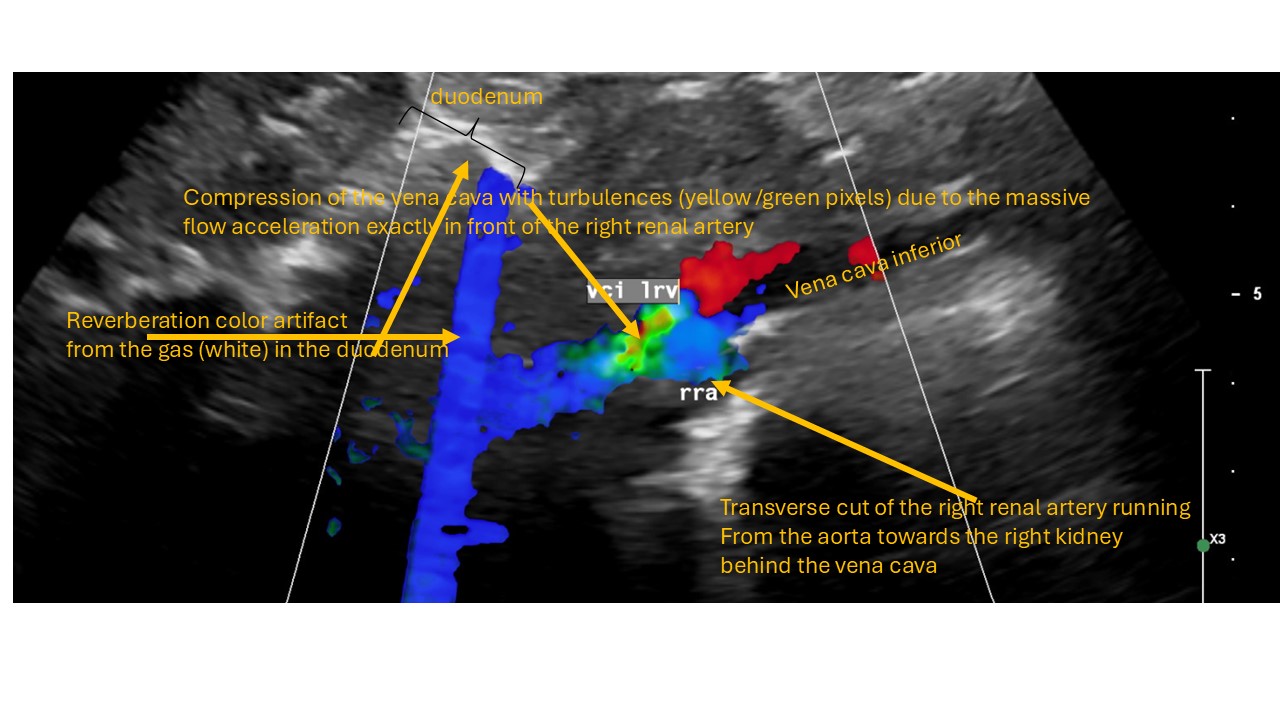
- compression of the vena cava by the right renal artery

- Post-prandial compression of the vena cava by the enlarging descending portion of the duodenum
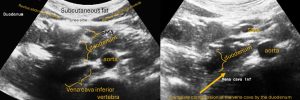
- Typically around 30-60 minutes after the uptake of food pain is produced by the conflict between the filling small bowel loops and the vena cava in the lower abdomen. Not only the blood flow inside the vena cava may become impaired but also the propulsion of the food may be hampered due to the restricted space in the lower abdomen in front of the protruding spine.

- in patients with a interruption of the peristaltic wave progression from the descending towards the horizontal portion of the duodenum

- In patients with Wilkie syndrome-obstruction of the horizontal portion of the duodenum
- Varying compression of the vena cava by the diaphragm depending on the respiratory position of the diaphragm











The treatment of these conditions is not easy and sometimes unexpected changes occur.
The easiest way to influenced congestion of the vena cava is a changing body posture.
- If the symptoms occur while lying supine-on the back-it is helpful to turn to the left side and flex the hips
- If the symptoms occur only while standing is helpful to sit down lifting the feet
- If the symptoms occur after a meal it is helpful to turn to the left side while lying horizontally
- It is always helpful to flex the hips or to pull the knees towards the chest while sitting
- It might be helpful to reduce the filling of the gastrointestinal tract by ingest small meals frequently
- It might be helpful to wear a corsage or compressive tights to prevent the downsinking of the abdominal organs, especially the liver
In selected cases an operation to decompress the vena cava might be contemplated.