- Praktyka medyczna
- Zespoły ucisku naczyniowego
- Czy masz jakieś pytania?
- Lista kontrolna Syndromy ucisku naczyniowego
- Charakterystyka układu mięśniowo-szkieletowego dojrzewania płci żeńskiej
- Lordozy / wydrążone plecy – Przyczyna licznych zespołów ucisku brzucha
- Zespół „dziadka do orzechów” jest błędną nazwą
- Zespół Midline (przeciążenie narządów linii środkowej)
- Zespół przeciążenia miednicy (przeciążenie organów miednicowych)
- Truncus coeliacus compression / Dunbar syndrome / MALS / Ligamentum arcuatum syndrome
- Zespół Wilkiego / zespół mezentryczny (arteria mesenterica superior)
- Kwantyfikacja zespołów ucisku naczyniowego przy użyciu techniki PixelFlux
- Neuralgia nadbrzusza w zespołach kompresji naczyniowej
- Leczenie zespołów ucisku naczyniowego
- Niedawno odkryte zespoły ucisku naczyniowego
- Funkcjonalne kolorowe ultradźwięki dopplerowskie – jak ja to robię
- Durchblutungsmessung – PixelFlux-Verfahren
- Badania
- Ekspertyza
- Zakażenie wirusem Bornavirusa
- Współpraca naukowa
- Cookie Policy
- Cookie Policy (EU)
Diaphragmatic compression of the hepatic veins
Here I describe a novel compression syndrome which I detected recently in a number of patients-the variable compression of the hepatic veins by the diaphragm during respiration.
Within the last year I saw multiple patients with complaints in the right upper abdomen-pain , tension, fullness related to this diaphragmatic hepatic vein compression .
In these patients I saw a venous outflow obstruction from the liver which in some of the patients’ caused and intermittent swelling of the liver which may be the reason for the above-mentioned complaints.
An outflow obstruction of the hepatic veins at their confluence into the vena cava inferior your is a well known entity called Budd-Chiari syndrome. This is usually caused by a thrombotic obstruction of this confluence or by fibrous ligaments or membranes which are thought to stem from the embryonic development of these veins and rarely due to other reasons.
So far unknown yet is a compression of these veins by the diaphragm which I detected in a number of patients by means of functional colour Doppler ultrasound.
In these patients turbulences are found at the confluence of the hepatic veins directly in front of their entrance into the vena cava inferior. These turbulences are caused by a narrowing of the hepatic veins producing an accelerated flow. This is a general sonographic hallmark of a Budd-Chiari syndrome.
In contrast to known pathologies producing a Budd-Chiari syndrome in the patient’s I observed this constriction of the hepatic veins was not constant but respiratory dependent. The degree of the constriction varied with inspiration and expiration. With this respect this newly detected compression syndrome resembles the median arcuate ligament syndrome.
In the median arcuate ligament syndrome (MALS) the aortic hiatus compresses the coeliac plexus and trunk from above by means of the sharp median arcuate ligament bridging the left and right diaphragmatic crus.
In the diaphragmatic compression of the hepatic veins mechanism is very similar. The passage of the vena cava from the abdominal cavity into the thorax is possible due to an opening in the diaphragm which resembles the aortic hiatus.
{kind=link}
In some patients the movement of the diaphragm from its inspiratory to its expiration position cuts into the confluence of the hepatic veins. This produces a variable narrowing of this confluence with a subsequent turbulent flow acceleration and venous congestion of the liver. Depending on the degree and duration of this compression a venous outflow obstruction of the liver a result producing a swelling of the liver (hepatomegaly) with ensuing pain in the right upper abdomen, tenderness and fullness.
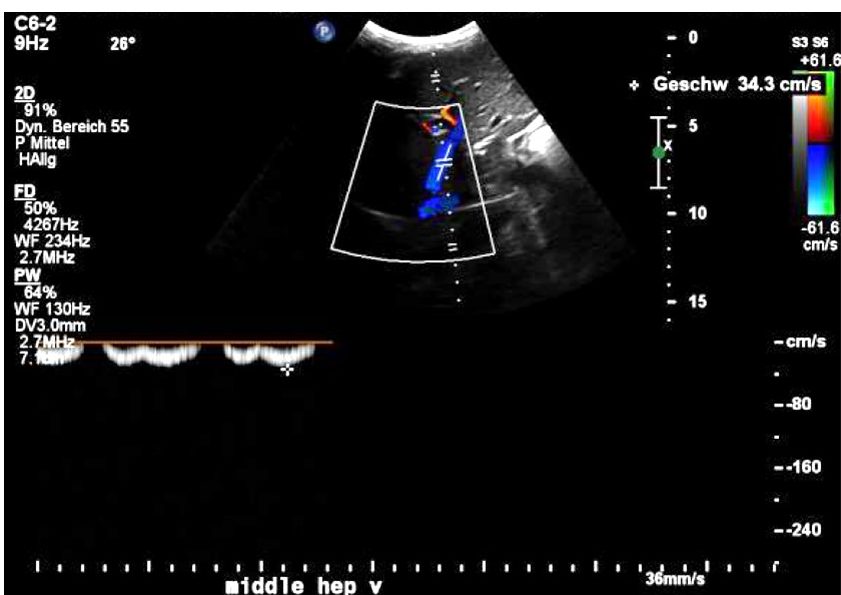
Normal blood flow within the central portion of the middle hepatic vein inside the liver with a maximum flow velocity of 34 cm/s.
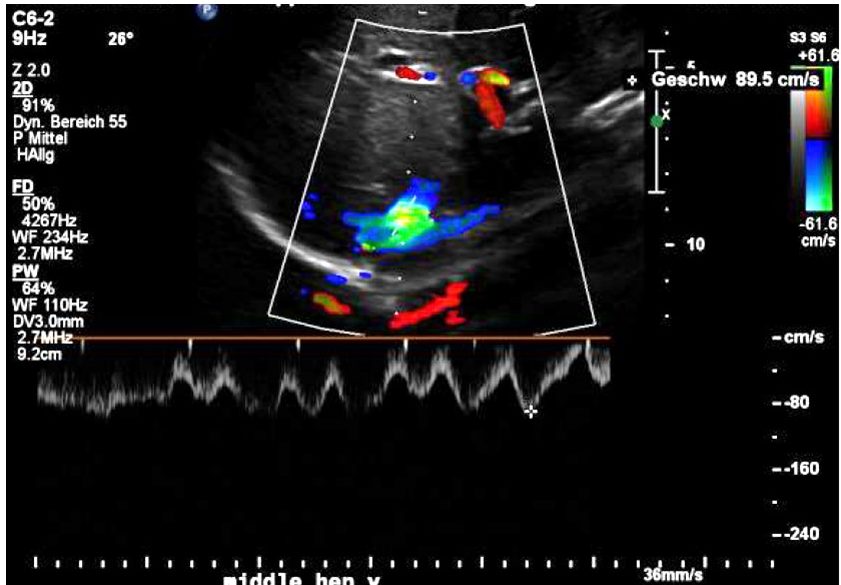
Significantly accelerated blood flow within the middle hepatic vein at the confluence with the vena cava inferior resulting in a turbulent flow acceleration (green pixels) and a maximum flow velocity of 89 cm/s.
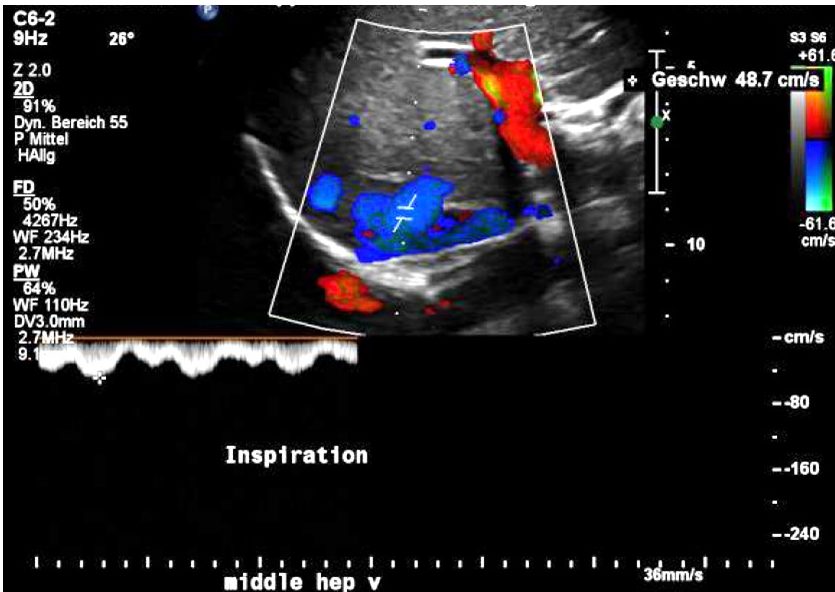
Sharp reduction of the flow velocity within the middle hepatic vein at the confluence during inspiration with a flow velocity dropping to 49 cm/s.
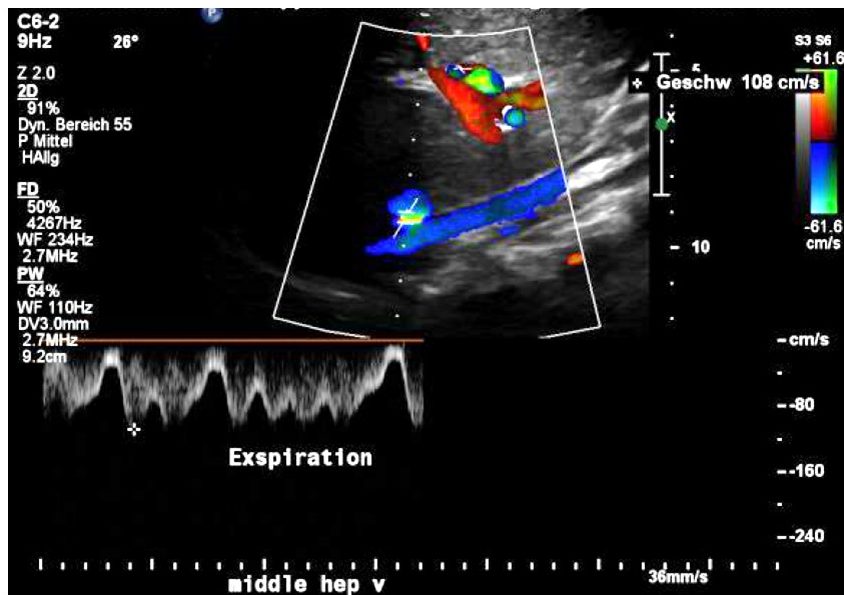
In expiration due to the compression of the confluence of the hepatic veins the flow suddenly accelerates to 108 cm/s.