- New stuff to read and discuss
- What patients say
- Clinic / online appointments
- Why the diagnosis of a psychosomatic illness is often a misdiagnosis
- Vascular Compression Syndromes
- Do you have questions?
- Checklist vascular compression syndromes
- Description of your symptoms
- Researchers from the Mayo Clinic confirm my concept of the Midline Congestion Syndrome
- Explanation of gender-specific differences in the clinical symptoms of abdominal vascular compression syndromes: varicocele and penile/testicular pain – their main manifestation in men.
- Varicocoele is predominantly caused by left renal vein compression
- Musculoskeletal pecularities of female puberty
- Lordosis /Swayback- Origin of many abdominal compression syndromes
- Bending of a straight vein compels its narrowing
- The lordogenetic midline congestion syndrome
- Neurological consequences of the midline congestion syndrome
- Successful treatment of a teenage girl who was unable to eat due to extreme postprandial pain and unable to walk due to spasticity in her left leg
- Severe ataxia in a young woman with severe spinal congestion – complete resolution after decompression of the left renal vein
- All compression syndromes are one: the spectrum of lordogenetic compressions
- Nutcracker-Syndrome is a misnomer! Lordogenetic left renal vein compression is a more appropriate name!
- May-Thurner-constellation (May-Thurner-syndrome, Cockett’s syndrome)
- Midline (congestion) syndrome
- Pelvic congestion syndrome
- Celiac Trunk Compression / Dunbar syndrome / MALS / Arcuate ligament syndrome
- Wilkie-Syndrome / Superior-mesenteric-artery-syndrome
- Compression of the vena cava inferior
- Evlauation of vascular compressions with the PixelFlux-method
- Connective tissue disorders predispose to multiple compressions
- Postural tachycardia syndrome (POTS) – the hemodynamic consequence of vascular compression syndromes and loose connective tissue
- Restless legs-a little known symptom of abdominal vascular compression syndromes
- Pudendal neuralgia in vascular compression syndromes
- A new sonographic sign of severe orthostatic venous pooling
- Migraine and Multiple Sclerosis
- Hemodynamic effect on cerebral perfusion in patients with multiple localised vascular compression.
- Treatment of vascular compression syndromes
- Fatal errors in the treatment of vascular compression syndromes
- Risks of stents in venous compression syndromes
- Surgical treatment of abdominal compression syndromes: The significance of hypermobility‐related disorders
- Nutcracker and May-Thurner syndrome: Decompression by extra venous tube grafting and significance of hypermobility related disorders
- Our surgical treatment of vascular compressions
- Chronic regional pain syndrome (CRPS) caused by venous compression and mechanical irritation of the coeliac plexus
- Vascular compression syndromes and other disease mechanisms I recently detected
- Kaleidoscope of instructive cases
- Venous congestion of the spinal cord may be a potential contributor to the development of paraplegia in patients with spinal muscular atrophy type III (Kugelberg-Welander disease)
- Ultrasound Diagnostics
- A breakthrough in functional sonographic diagnostic – 4D-colour Doppler sonographic flow volume measurements
- 4D-volume flow measurements of jugular and mesenteric veins
- Inauguration of the global volumetric brain perfusion measurement-a gateway for understanding of neurological symptoms
- Ultrasound focused entirely on all of your symptoms
- Ultrasound vs. X-ray
- Vascular Malformations
- Profile
- Functional colour Doppler ultrasound – how I do it
- Perfusion Measurement – PixelFlux-method
- Research
- Publications
- Nutcracker and May-Thurner syndrome: Decompression by extra venous tube grafting and significance of hypermobility related disorders
- Papers authored by Th. Scholbach
- Publications
- Inauguration of measurements of the tissue pulsatility index in renal transplants
- From nutcracker phenomenon to midline congestion syndrome and its treatment with aspirin
- First sonographic tissue perfusion measurement in renal transplants
- First sonographic bowel wall perfusion measurement in Crohn disease
- First sonographic renal tissue perfuison measurement
- First sonographic measurement of renal perfusion loss in diabetes mellitus
- PixelFlux measurements of renal tissue perfusion
- Why I prefer not to publish in journals but in the Internet
- Vessel stretching in nephroptosis – an important driver of complaints
- Publications
- Expertise
- Bornavirus Infection
- Scientific cooperation
- Cookie Policy
- Data protection
- Cookie Policy (EU)
- Impressum
Muscle cramps caused by a posture dependent pubic compression of the femoral artery
An erect stance causes an anterior tilt of the pelvis due to the anatomy of the human hip joint. Ligaments restrict a stretching of the hip joints above an angle of about 45° less than the full stretching. This was detected by my father, Dr. Manfred Scholbach, who researched on the so-called restricted hip stretching of newborns. He described for the first time that in newborn babies the femur always has an angle of about 90-130° with the horizontal plane when the babies lie on their back. A passive stretching of a newborn’s hip to align the femur with the spine inevitably causes a tilting of the entire pelvis producing an elevation of the sacral bone and caudal lumbar spine. Thus, he claimed and confirmed that a full stretching of the hip is achieved when the femur has an angle with the horizontal line of about 45° while the patient is in a supine position.
Only later in childhood after they begin to walk children acquire the ability to align their upper thighs with the direction of the spine. But this requires and anterior tilt of the pelvis. This tilting, in addition to the effect of gravity on the upright spine, is responsible for the lumbar lordosis of the human spine, which is not an inborn feature of the human anatomy but an acquired one.
The range of motion of the hip joint of a human being is similar to that of quadruped animals. Observing a running dog or a horse illustrates the above explained research. These animals , even during a full speed race never raise the hind legs to a horizontal line. But this would correspond to the achievement of a full hip stretching as it is typical for human beings beyond the age of 1 year.
The full hip stretching thus pulls the blood vessels and nerves at the ventral surface of the upper thigh across the pubic bone. If humans would walk on 4 legs as quadruped animals do such a stretching would be omitted.
I demonstrate here for the first time a so far (2021 09 11 ) undescribed effect of a pathologic stretching of the femoral artery across the pubic bone in a lady of 87 years who developed a painful reduction of her walking distance. After about 500 m she regularly complained about pain in her right calf which prompted her to sit down and rest. Sometimes painful muscle cramps occurred sometimes only a dull pain developed. There was no swelling of the leg and no discoloration, nor a bluish or a pale one.
Examinations of her electrolyte metabolism, blood pressure measurements in both legs and neurologic examinations did not reveal any abnormality.
The blood flow measurements in her right and left leg as well as in the aorta and the right iliac arteries revealed a dampened pulse-wave throughout the entire right leg while the patient was lying supine with stretched hips. There was no stenosis within the aorta nor the iliac arteries on the right side. No stenotic changes in the right femoral, popliteal, and tibial arteries nor in the arteries of the right foot could be demonstrated.
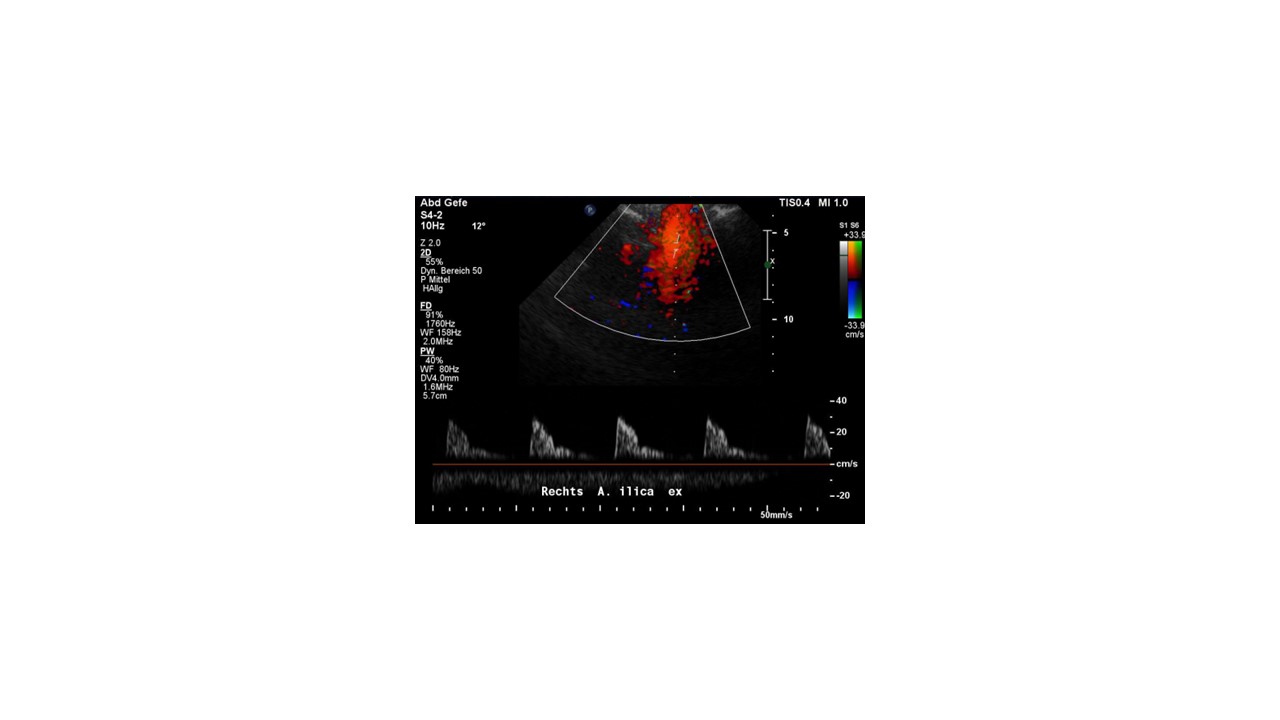
Normal flow pattern in the right external iliac artery with a steep systolic flow acceleration while lying with stretched hips – no poststenotic flow pattern

Normal flow pattern in the right common iliac artery, ruling out a stenosis of the aorta or the right common iliac artery artery, no arteriosclerosis
Nevertheless, it was impressive that the blood flow volume in the dorsal artery of the left foot was 29 mL/min whereas in the right foot it was only 9 mL/min in a supine position with stretched hips.
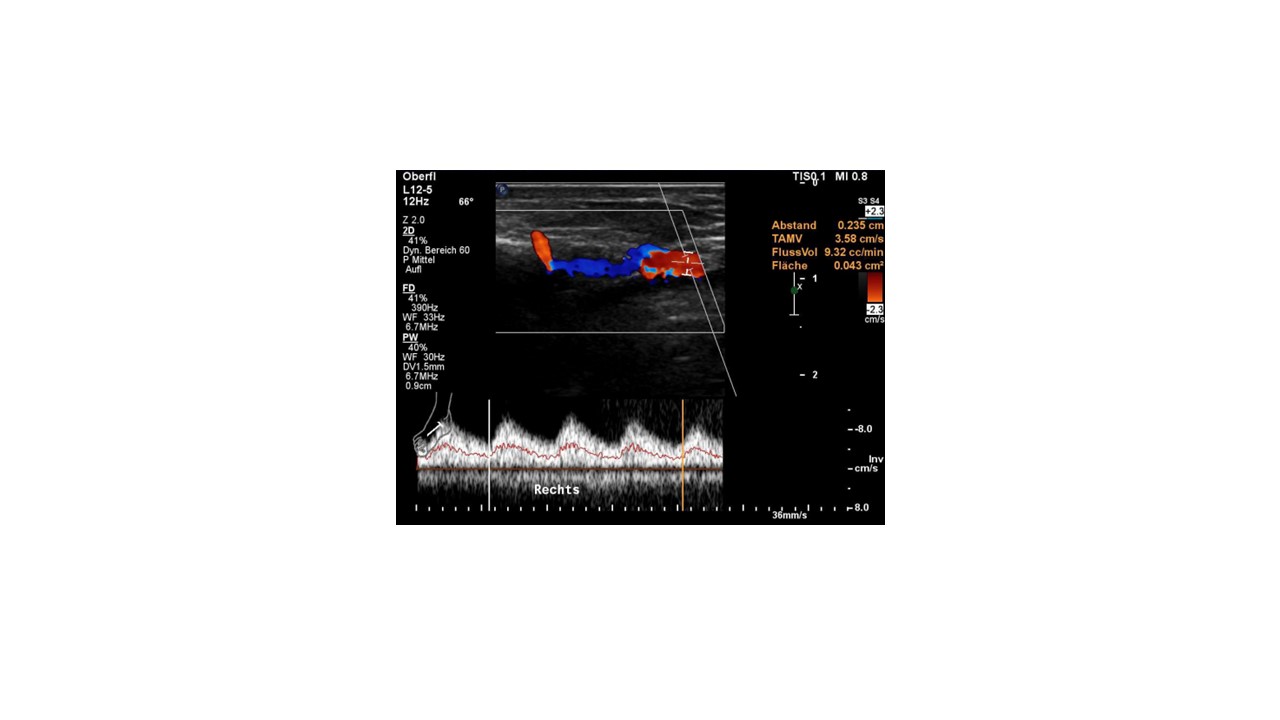
The diastolic flow velocity in the right dorsal artery of the food is relatively high. This is a sign of dilatation of the blood vessels to exhaust the remaining blood flow volume in severe ischaemia of the entire leg. This cannot compensate for the severe drop of blood flow volume to only 9.32 mL/min which underscores to severity of the ischaemia while the hips are stretched.

In comparison to the right foot, the left foot has a normal arterial perfusion with only little diastolic flow but a much higher flow volume: 26.6 mL/min. The left femoral artery is not compressed contrary to the right one.
After flexing the hip and putting the right foot flat onto the examination bed the blood flow pattern in the right leg normalized and so did the blood flow volume in the right foot.

The blood flow pattern in the right femoral artery shows a very slow increase of the flow velocity from the beginning to the peak of the cyst only. This lasts 209 ms due to the dampening of the pulse-wave by the pubic bone which compresses the right femoral artery nearly completely

After flexing the hip the blood flow pattern in the femoral artery improves immediately. The time to reach the peak of the systolic wave reduces from 209 to only 44 ms. This is a clear sign of the variable decompression and compression of the femoral artery by the pubic bone, dependent on the angulation of the hip joint.
A variable compression of the right femoral artery by the pubic bone could be demonstrated as the reason for the disturbed arterial perfusion of the entire right leg in body postures with stretched hips.
The flow signal significantly changed from a normal one above the pubic bone on the right side to a slowly increasing systolic blood flow with a dampened height of the maximum flow velocity below the pubic bone in the arteries of the right leg as long as the patient stretched her hips.
This corresponded very well to her clinical description of a painful reduction of her maximum walking distance. While being upright the perfusion of her right calf was reduced to one third of the left calf. This led to an ischemia, recognizable as a relatively increased diastolic flow velocity to exhaust the oxygen from the remaining perfusion volume. The ischemia caused muscle cramping and pain while walking.
Since during sitting the hips are flexed a restoration of the blood flow volume occurs and the pain subsides.
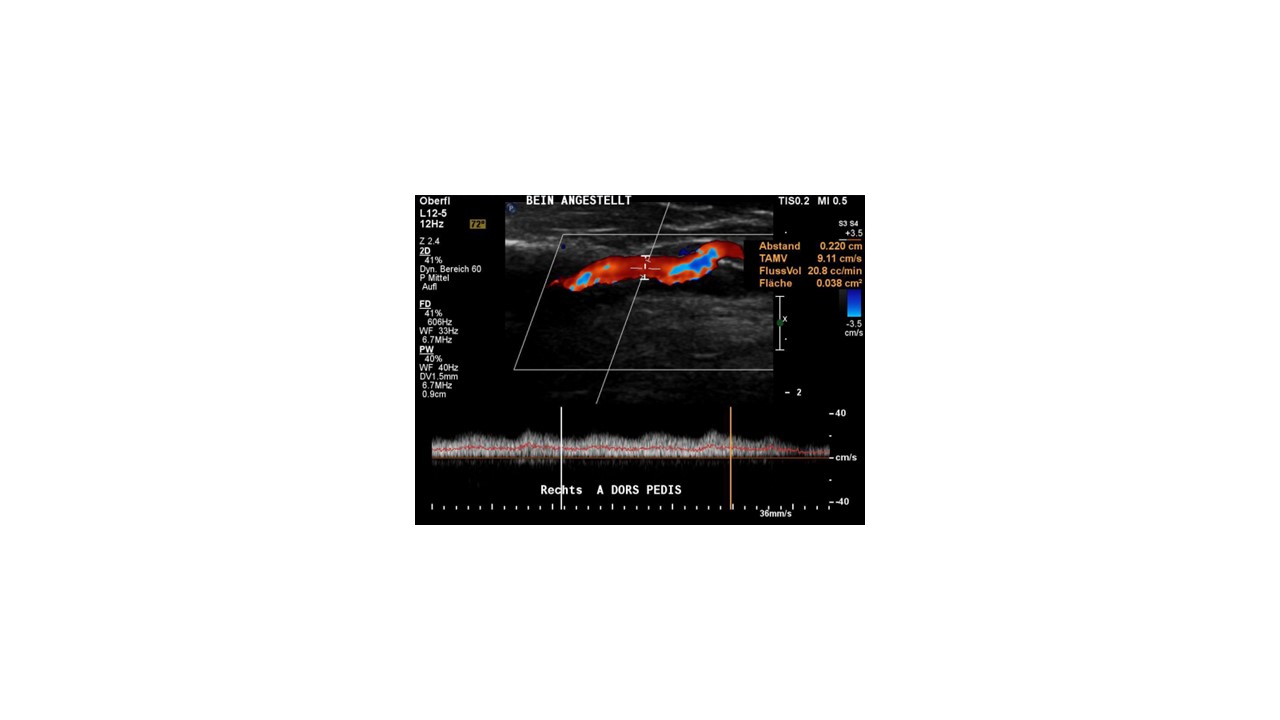
After flexing the hip, suddenly the blood flow volume in the right food and the entire right leg turns to near normal: 20.8 mL/min compared to 26.6 mL/min on the left side.
Only a qualitative flow volume measurement could depict the true severity of the variable compression of the right femoral artery which reduced the entire blood flow volume to one third. Simple flow velocity measurements would substantially underestimate the degree and thus the clinical impact of this peculiar mobile arterial compression syndrome.