- New stuff to read and discuss
- What patients say
- Clinic / online appointments
- Why the diagnosis of a psychosomatic illness is often a misdiagnosis
- Vascular Compression Syndromes
- Do you have questions?
- Checklist vascular compression syndromes
- Description of your symptoms
- Researchers from the Mayo Clinic confirm my concept of the Midline Congestion Syndrome
- Explanation of gender-specific differences in the clinical symptoms of abdominal vascular compression syndromes: varicocele and penile/testicular pain – their main manifestation in men.
- Varicocoele is predominantly caused by left renal vein compression
- Musculoskeletal pecularities of female puberty
- Lordosis /Swayback- Origin of many abdominal compression syndromes
- Bending of a straight vein compels its narrowing
- The lordogenetic midline congestion syndrome
- Neurological consequences of the midline congestion syndrome
- Successful treatment of a teenage girl who was unable to eat due to extreme postprandial pain and unable to walk due to spasticity in her left leg
- Severe ataxia in a young woman with severe spinal congestion – complete resolution after decompression of the left renal vein
- All compression syndromes are one: the spectrum of lordogenetic compressions
- Nutcracker-Syndrome is a misnomer! Lordogenetic left renal vein compression is a more appropriate name!
- May-Thurner-constellation (May-Thurner-syndrome, Cockett’s syndrome)
- Midline (congestion) syndrome
- Pelvic congestion syndrome
- Celiac Trunk Compression / Dunbar syndrome / MALS / Arcuate ligament syndrome
- Wilkie-Syndrome / Superior-mesenteric-artery-syndrome
- Compression of the vena cava inferior
- Evlauation of vascular compressions with the PixelFlux-method
- Connective tissue disorders predispose to multiple compressions
- Postural tachycardia syndrome (POTS) – the hemodynamic consequence of vascular compression syndromes and loose connective tissue
- Restless legs-a little known symptom of abdominal vascular compression syndromes
- Pudendal neuralgia in vascular compression syndromes
- A new sonographic sign of severe orthostatic venous pooling
- Migraine and Multiple Sclerosis
- Hemodynamic effect on cerebral perfusion in patients with multiple localised vascular compression.
- Treatment of vascular compression syndromes
- Fatal errors in the treatment of vascular compression syndromes
- Risks of stents in venous compression syndromes
- Surgical treatment of abdominal compression syndromes: The significance of hypermobility‐related disorders
- Nutcracker and May-Thurner syndrome: Decompression by extra venous tube grafting and significance of hypermobility related disorders
- Our surgical treatment of vascular compressions
- Chronic regional pain syndrome (CRPS) caused by venous compression and mechanical irritation of the coeliac plexus
- Vascular compression syndromes and other disease mechanisms I recently detected
- Kaleidoscope of instructive cases
- Venous congestion of the spinal cord may be a potential contributor to the development of paraplegia in patients with spinal muscular atrophy type III (Kugelberg-Welander disease)
- Ultrasound Diagnostics
- A breakthrough in functional sonographic diagnostic – 4D-colour Doppler sonographic flow volume measurements
- 4D-volume flow measurements of jugular and mesenteric veins
- Inauguration of the global volumetric brain perfusion measurement-a gateway for understanding of neurological symptoms
- Ultrasound focused entirely on all of your symptoms
- Ultrasound vs. X-ray
- Vascular Malformations
- Profile
- Functional colour Doppler ultrasound – how I do it
- Perfusion Measurement – PixelFlux-method
- Research
- Publications
- Nutcracker and May-Thurner syndrome: Decompression by extra venous tube grafting and significance of hypermobility related disorders
- Papers authored by Th. Scholbach
- Publications
- Inauguration of measurements of the tissue pulsatility index in renal transplants
- From nutcracker phenomenon to midline congestion syndrome and its treatment with aspirin
- First sonographic tissue perfusion measurement in renal transplants
- First sonographic bowel wall perfusion measurement in Crohn disease
- First sonographic renal tissue perfuison measurement
- First sonographic measurement of renal perfusion loss in diabetes mellitus
- PixelFlux measurements of renal tissue perfusion
- Why I prefer not to publish in journals but in the Internet
- Vessel stretching in nephroptosis – an important driver of complaints
- Publications
- Expertise
- Bornavirus Infection
- Scientific cooperation
- Cookie Policy
- Data protection
- Cookie Policy (EU)
- Impressum
Non-pulsatile bilateral tinnitus that intensifies when turning the head to the left in a patient with compression of the left renal vein and left internal jugular vein.
The 61-year-old male patient has suffered from continuous bilateral tinnitus for four years. A distinctive feature is that the volume of the tinnitus increases significantly when the patient turns their head to the left. The patient also experiences nasal congestion in the mornings.
Diagnostic tests indicated cerebral congestion due to compression of both the left renal vein and the left internal jugular vein.
Tinnitus can develop when venous blood cannot drain properly from the skull[1], while the arterial inflow remains unaffected.
This leads to a chronic increase in venous pressure inside the skull[2], the tangible expression of which is morning swelling of the nasal mucous membranes. This regularly occurs when intracranial pressure rises, as blood is released from the veins of the nasal mucosa into the interior of the skull via an anastomosis between the angular vein of the nose and the superior ophthalmic vein. This connects the facial vein and the cavernous sinus within the skull. If venous pressure inside the skull is too high, blood accumulates in the nasal mucosa, impairing nasal breathing.
A characteristic feature of patients with vascular compression syndromes is that the swelling of the nasal mucosa disappears approximately one hour after waking up. Patients with abdominal vascular compression experience a shift of the congested venous blood into the spinal canal at night, causing increasing pressure to be transmitted intracranially via the cerebrospinal fluid. This leads to compression of the intracranial veins.
Intracranial pressure fluctuations depending on body position can also be detected in healthy individuals. However, in patients with impaired venous drainage from the skull, these fluctuations are clinically noticeable, initially manifesting as swelling of the nasal mucosa.
In my experience, headaches then regularly occur later on in such patients, and functional disorders of the brain stem are not uncommon. These include snoring due to relaxation of the soft palate (its muscles are innervated by the 9th and 10th cranial nerves), nocturnal teeth grinding (masticatory muscles innervated by the 5th cranial nerve) and motor speech disorders (tongue innervated by the 12th cranial nerve).
In this context, it is interesting to recall the location of the cranial nerve nuclei:
| Cranial Nerve | Name | Location in the brain stem |
| III | N. oculomotorius | Midbrain (mesencephalon) |
| IV | N. trochlearis | Midbrain (mesencephalon) |
| V | N. trigeminus | Midbrain, pons, medulla oblongata, spinal cord |
| VI | N. abducens | Pons (bridge) |
| VII | N. facialis | Pons (bridge) |
| VIII | N. vestibulocochlearis | Pons / medulla oblongata |
| IX | N. glossopharyngeus | Medulla oblongata (elongated medulla) |
| X | N. vagus | Medulla oblongata (elongated medulla) |
| XI | N. accessorius | Medulla oblongata & upper spinal cord |
| XII | N. hypoglossus | Medulla oblongata (elongated medulla) |
The table shows that the nuclei of cranial nerves responsible for te above mentioned symptoms are located in the medulla oblongata, which is the deepest lying part of the brain.
Just as venous blood collects at the lowest points of the torso (the small pelvis) and the legs (the feet) in abdominal and pelvic venous compression syndromes, the posterior cranial fossa, containing the medulla oblongata, acts as a barrier similar to the bony pelvic ring. This barrier does not completely prevent the descent of venous blood, but it does impede it. This can lead to blood collecting preferentially in the posterior cranial fossa when intracranial pressure is exerted on the brain’s veins, causing functional disorders of the cranial nerve nuclei located in the medulla oblongata — the lowest part of the brain in the posterior cranial fossa[3, 4].
This is one possible explanation for the development of functional disorders of the auditory nerve (the 8th cranial nerve, or vestibulocochlear nerve). Functional disorders here can lead to tinnitus. Therefore, tinnitus can be alleviated in these cases by reducing or eliminating venous congestion in the brain.
However, this requires accurate measurement of the venous outflow from the skull. This is not possible using standard diagnostic procedures such as extracranial and transcranial sonography, CT and MRI.
The rationale behind the quantitative determination of venous drainage from the skull is to use 4D PixelFlux volume flow measurements of the internal jugular vein. The internal jugular vein is the brain’s most important drainage pathway. Compression of this vessel is therefore particularly significant. The other two drainage pathways are the vertebral veins and the epidural plexus veins. However, these drainage pathways are limited by the bony structures of the spine. The vertebral veins run through the bone rings of the lateral processes of the cervical vertebrae and cannot therefore expand significantly when there is an increase in volume. Similarly, the veins of the epidural plexus cannot expand freely as they are located within the spinal canal.
If the internal jugular vein is significantly compressed, the other two drainage pathways may reach their capacity limits.
However, if the epidural plexus is already full and exhausted due to blood flowing in from the left renal vein in nutcracker syndrome or the left pelvic vein in May–Thurner syndrome — whereby instead of draining blood from the skull, it supplies blood to the inside of the skull — then compression of the internal jugular vein can easily lead to clinical symptoms.
I will describe how quantitative perfusion measurement of the involved veins can provide clues to the development of tinnitus using the example of non-pulsatile tinnitus, which increased in volume when the head was turned to the left.
The patient had severe compression of the left internal jugular vein.


The right internal jugular vein was compressed too, but apparently to a lesser extent.
Both the reduction in the calibre of the vein and the acceleration of flow were significantly greater on the left side than on the right.


Volume flow measurements provide a much more reliable indication. They adequately describe the function of a vessel — transporting a certain volume of blood — whereas assessments of vessel diameter and flow velocity can only provide vague indications of impaired volume transport. Determining the diameter of veins is particularly problematic as they are often irregularly shaped, especially in the neck. Furthermore, they constantly change with breathing, body posture or due to the pulse of neighbouring arteries. Therefore, simple determinations of vein diameter are useless.
Determining the flow velocity alone is also unreliable. Flow velocity depends on the blood supply and the pressure gradient at the narrowing. With the same vessel narrowing, flow acceleration may be lower with a reduced blood supply — for example, after collateral veins have developed — than in the absence of collateral circulation.
Therefore, four-dimensional PixelFlux blood volume perfusion measurement significantly improves upon established methods in Doppler sonography, CT and MR angiography.
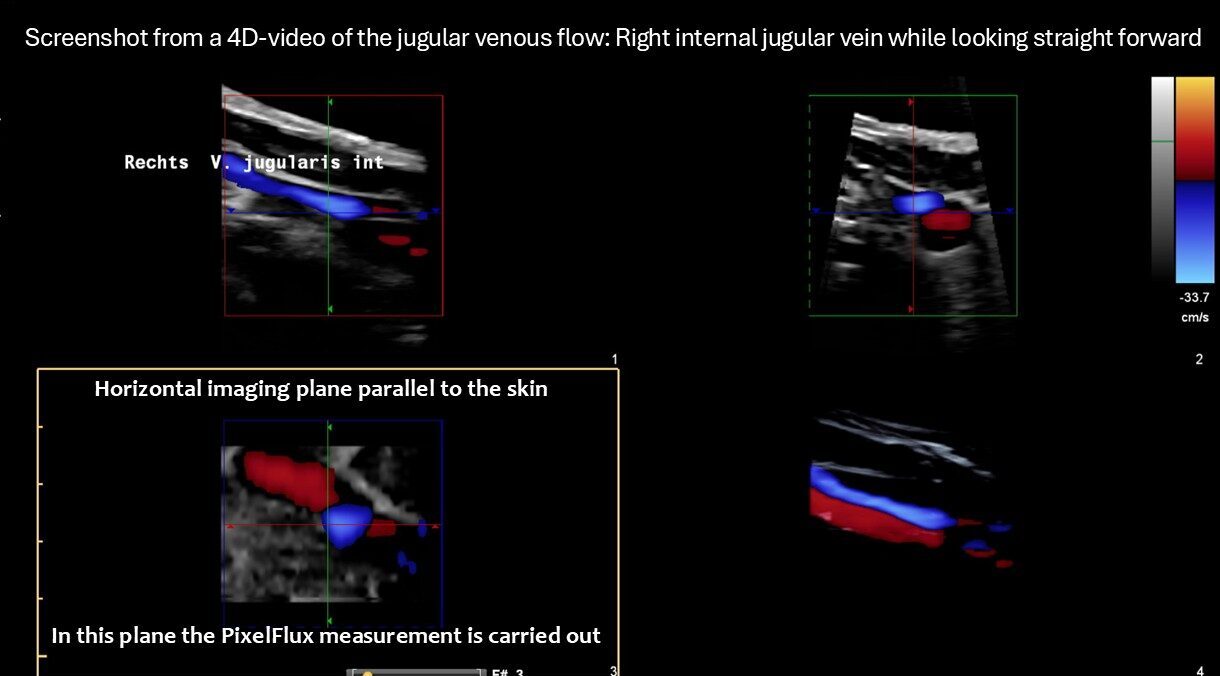

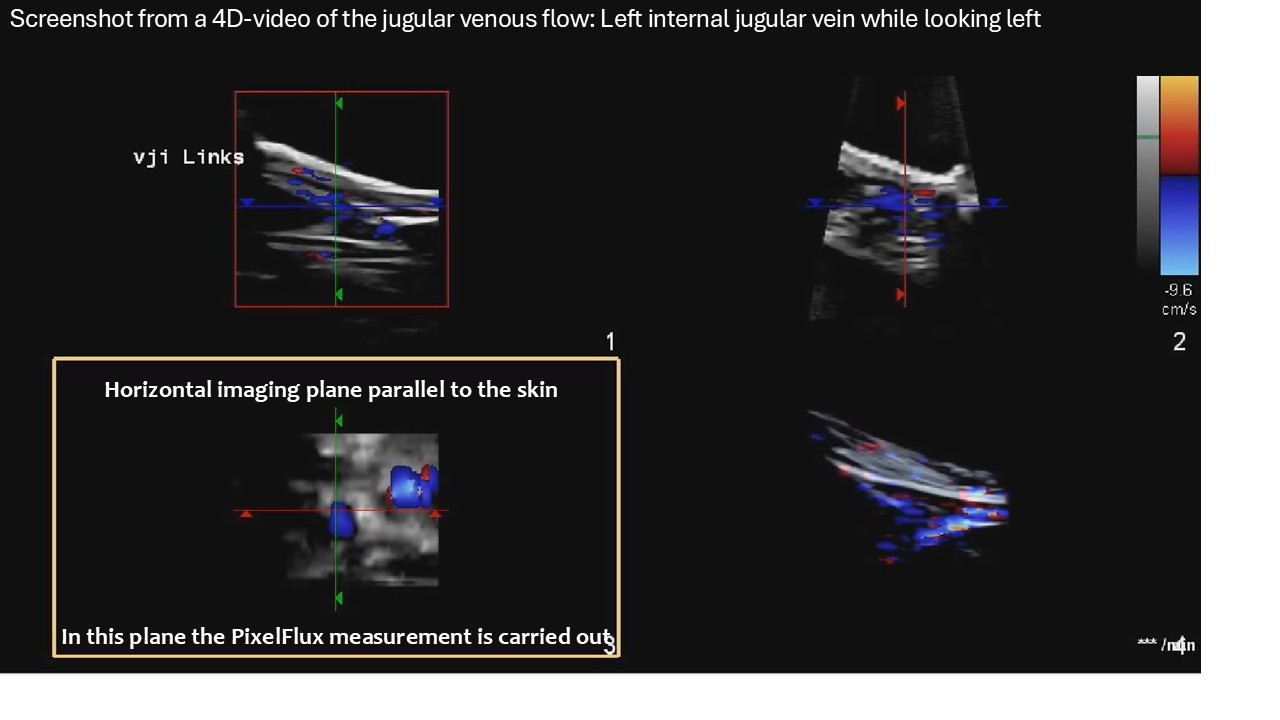

In this patient, 4D PixelFlux blood volume flow measurement of the jugular veins revealed a dramatic change on the left side when the patient turned their head to the left. This precisely increased the volume of the patient’s tinnitus.
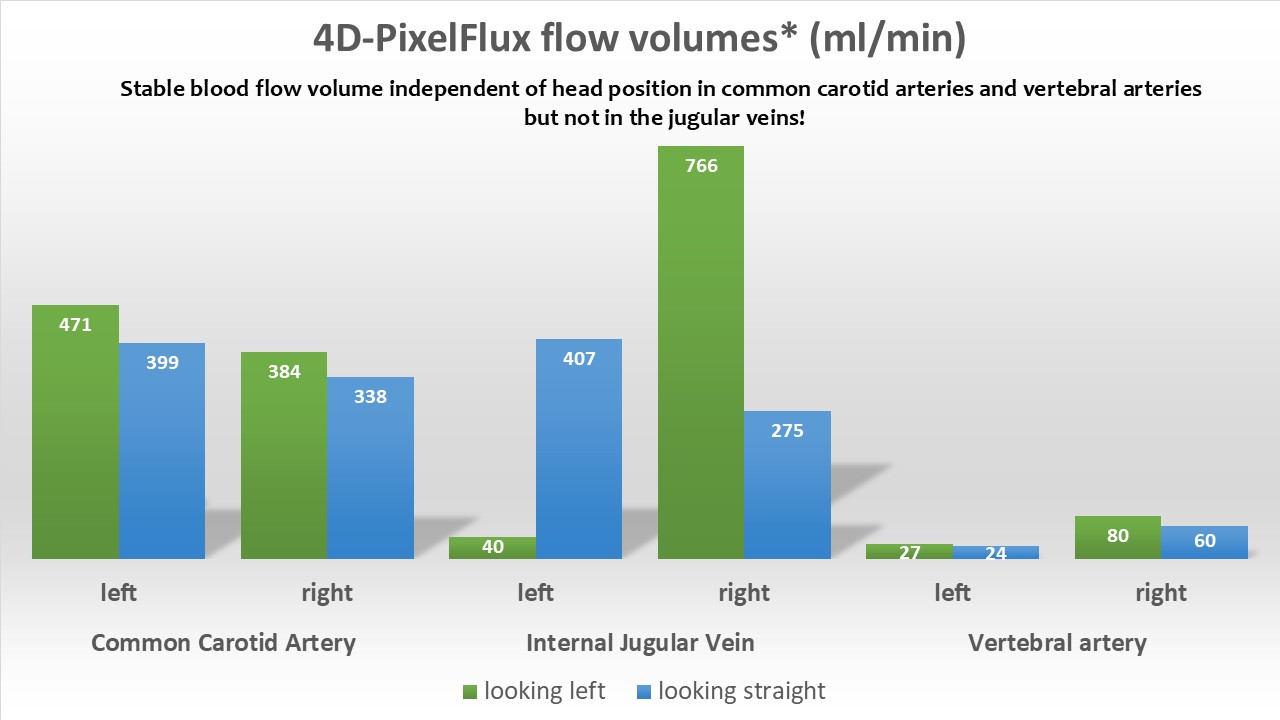
Additionally, PixelFlux measurement of renal perfusion revealed that changing the head position to look left resulted in a significant reduction in blood flow to the left kidney.
Colour duplex sonography revealed a nutcracker constellation of the left renal vein 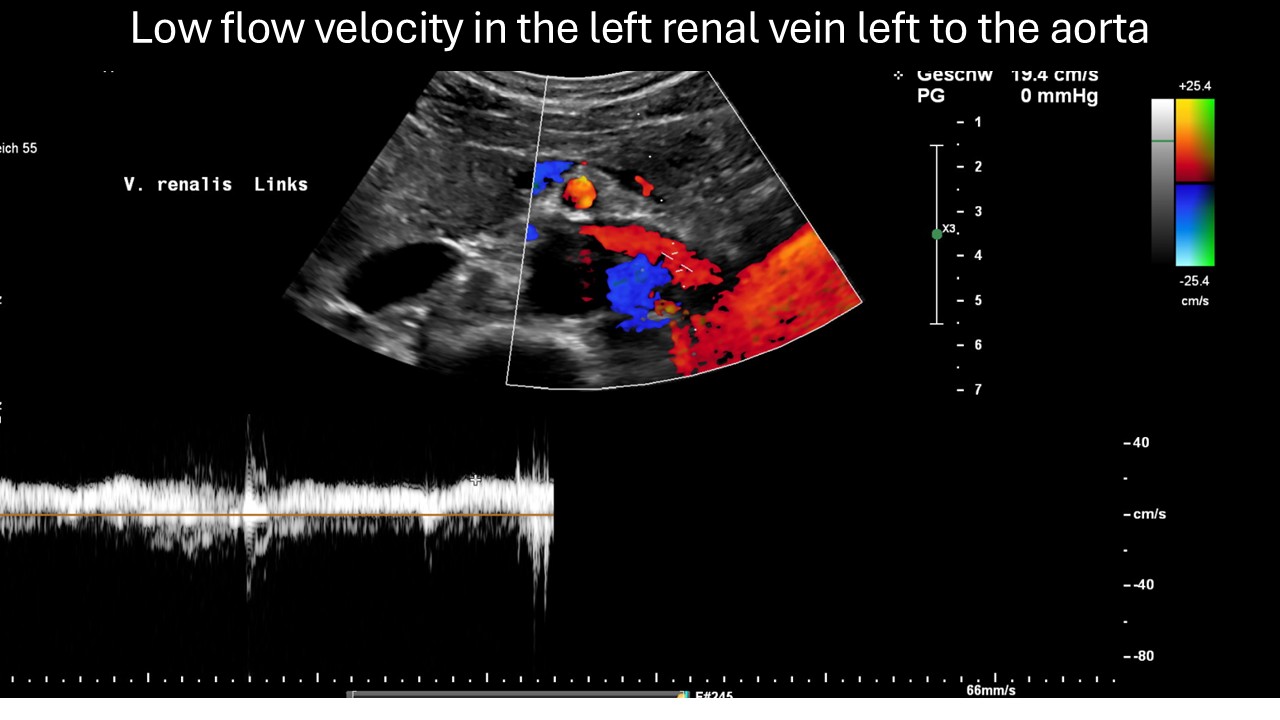

and a pelvic congestion with reversed flow in the left internal iliac vein:

and a strong venous connection from the spine to the left renal vein, known as a tronc réno-rachidien. This vessel serves to equalise pressure between the renal vein and the epidural plexus. The fact that blood flow to the left kidney was significantly lower than to the right kidney, even with normal head posture, indicates the inability of the collateral circulation to adequately drain congested blood from the left renal vein.


Due to communication between the renal vein and the tronc réno-rachidien, the epidural plexus was also involved in these collateral circulations.

If turning the head to the left suddenly deteriorates blood flow to the left kidney, this directly expresses the additional restriction of the collateral circulation via the epidural plexus. This restriction can be explained by an increase in pressure in the epidural plexus, triggered by turning the head to the left. Turning the head to the left was shown to significantly reduce blood flow in the left internal jugular vein in the 4D PixelFlux measurement. This indicates that, when the head was turned to the left, blood could no longer flow to the heart via the left jugular vein and had to find an alternative route via the epidural plexus. This leads to a significant increase in pressure in the spinal canal due to the additional amount of blood that would otherwise have flowed through the jugular vein. As a result of the increase in intraspinal pressure, blood flow to the left kidney deteriorates further, as the left kidney is now deprived of part of the capacity of its bypass circuits.
Thus, the functionally significant relationships between the various veins in the body, from the head to the pelvis and legs, can be visualised and quantitatively described. This can significantly contribute to assessing the origin of symptoms and advising on treatment.
Literature:
- Wei, H., et al., Cerebral venous congestion alters CNS homeostatic plasticity, evoking tinnitus-like behavior. Cell Biosci, 2024. 14(1): p. 47.
- Williams, H., The venous hypothesis of hydrocephalus. Med Hypotheses, 2008. 70(4): p. 743–7.
- Zhou, D., et al., Understanding jugular venous outflow disturbance. CNS Neurosci Ther, 2018. 24(6): p. 473–482.
- Zhou, D., et al., Clinical Characteristics and Neuroimaging Findings in Internal Jugular Venous Outflow Disturbance. Thromb Haemost, 2019. 119(2): p. 308–318.