- New stuff to read and discuss
- What patients say
- Clinic / online appointments
- Why the diagnosis of a psychosomatic illness is often a misdiagnosis
- Vascular Compression Syndromes
- Do you have questions?
- Checklist vascular compression syndromes
- Description of your symptoms
- Researchers from the Mayo Clinic confirm my concept of the Midline Congestion Syndrome
- Explanation of gender-specific differences in the clinical symptoms of abdominal vascular compression syndromes: varicocele and penile/testicular pain – their main manifestation in men.
- Varicocoele is predominantly caused by left renal vein compression
- Musculoskeletal pecularities of female puberty
- Lordosis /Swayback- Origin of many abdominal compression syndromes
- Bending of a straight vein compels its narrowing
- The lordogenetic midline congestion syndrome
- Neurological consequences of the midline congestion syndrome
- Successful treatment of a teenage girl who was unable to eat due to extreme postprandial pain and unable to walk due to spasticity in her left leg
- Severe ataxia in a young woman with severe spinal congestion – complete resolution after decompression of the left renal vein
- All compression syndromes are one: the spectrum of lordogenetic compressions
- Nutcracker-Syndrome is a misnomer! Lordogenetic left renal vein compression is a more appropriate name!
- May-Thurner-constellation (May-Thurner-syndrome, Cockett’s syndrome)
- Midline (congestion) syndrome
- Pelvic congestion syndrome
- Celiac Trunk Compression / Dunbar syndrome / MALS / Arcuate ligament syndrome
- Wilkie-Syndrome / Superior-mesenteric-artery-syndrome
- Compression of the vena cava inferior
- Evlauation of vascular compressions with the PixelFlux-method
- Connective tissue disorders predispose to multiple compressions
- Postural tachycardia syndrome (POTS) – the hemodynamic consequence of vascular compression syndromes and loose connective tissue
- Restless legs-a little known symptom of abdominal vascular compression syndromes
- Pudendal neuralgia in vascular compression syndromes
- A new sonographic sign of severe orthostatic venous pooling
- Migraine and Multiple Sclerosis
- Hemodynamic effect on cerebral perfusion in patients with multiple localised vascular compression.
- Treatment of vascular compression syndromes
- Fatal errors in the treatment of vascular compression syndromes
- Risks of stents in venous compression syndromes
- Surgical treatment of abdominal compression syndromes: The significance of hypermobility‐related disorders
- Nutcracker and May-Thurner syndrome: Decompression by extra venous tube grafting and significance of hypermobility related disorders
- Our surgical treatment of vascular compressions
- Chronic regional pain syndrome (CRPS) caused by venous compression and mechanical irritation of the coeliac plexus
- Vascular compression syndromes and other disease mechanisms I recently detected
- Kaleidoscope of instructive cases
- Venous congestion of the spinal cord may be a potential contributor to the development of paraplegia in patients with spinal muscular atrophy type III (Kugelberg-Welander disease)
- Ultrasound Diagnostics
- A breakthrough in functional sonographic diagnostic – 4D-colour Doppler sonographic flow volume measurements
- 4D-volume flow measurements of jugular and mesenteric veins
- Inauguration of the global volumetric brain perfusion measurement-a gateway for understanding of neurological symptoms
- Ultrasound focused entirely on all of your symptoms
- Ultrasound vs. X-ray
- Vascular Malformations
- Profile
- Functional colour Doppler ultrasound – how I do it
- Perfusion Measurement – PixelFlux-method
- Research
- Publications
- Nutcracker and May-Thurner syndrome: Decompression by extra venous tube grafting and significance of hypermobility related disorders
- Papers authored by Th. Scholbach
- Publications
- Inauguration of measurements of the tissue pulsatility index in renal transplants
- From nutcracker phenomenon to midline congestion syndrome and its treatment with aspirin
- First sonographic tissue perfusion measurement in renal transplants
- First sonographic bowel wall perfusion measurement in Crohn disease
- First sonographic renal tissue perfuison measurement
- First sonographic measurement of renal perfusion loss in diabetes mellitus
- PixelFlux measurements of renal tissue perfusion
- Why I prefer not to publish in journals but in the Internet
- Vessel stretching in nephroptosis – an important driver of complaints
- Publications
- Expertise
- Bornavirus Infection
- Scientific cooperation
- Cookie Policy
- Data protection
- Cookie Policy (EU)
- Impressum
Successful treatment of severe post-prandial upper abdominal pain due to pancreatic congestion in a patient with high-grade compression of the splenic vein
A 24-years old female patient had been operated to decompress the initially severely compressed left renal vein. Postoperatively she developed a compression of the splenic vein by the coeliac trunk against the prepyloric antrum of the stomach and a progressive left common iliac vein compression.
Her main complaints were unbearable post-prandial epigastric pain (severity 9/10) , back pain and she was unable to stand for longer periods.
For the past month, the patient has had 6 episodes of increasing pain located below the left ribcage and radiating to the spine on the left side. In addition, she experienced more pain while working and a different type of pain while eating. As a result, she lost about 10 pounds in the last 3 months by avoiding the uptake of food to reduce the pain.
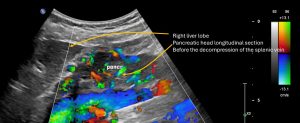
Prior to the operation the patient was suffering from severe post-prandially accentuated epigastric pain which could be referred to the massive congestion of the pancreas. The following videos demonstrate the hypervascular pancreatic head and pancreatic tail.
Preoperative sweep across the pancreas showing a massive vascularisation of the entire organ due to its involvement into the collateral pathway of the severely compressed splenic vein
Video showing the congested pancreatic head with a network of multiple intertwined congested veins. The extent of the congestion can only be measured with the PixelFlux technique-see below
Detailed post-operative view of the pancreatic head. The decompression of the splenic vein renders the collateral network in the pancreas unnecessary which thus disappears due to its collaps.
Vide showing the pancreatic tail after the decompression of the splenic vein-now no blood vessels can be depicted anymore inside the pancreas- a proof of the former involvement of the pancreas in the collateral pathway of the compressed splenic vein
Close up view of the former compression site of the splenic vein at the crossing with the coeliac trunk after its decompression
Worm- like intertwining enlarged parenchymal veins inside the head of the pancreas due to its involvement in the collateral pathway of the compressed splenic vein prior to the surgical decompression

After surgical decompression of the splenic vein the venous collateral network inside the pancreatic head completely disappeared. A clear. the pancreas was involved in the collateral pathway of the compressed splenic vein.
The only way to quantify the extent of the collateralisation of a parenchymal organ by means of ultrasound-which is obviously the most patient-friendly imaging technique-is the PixelFlux measurement:
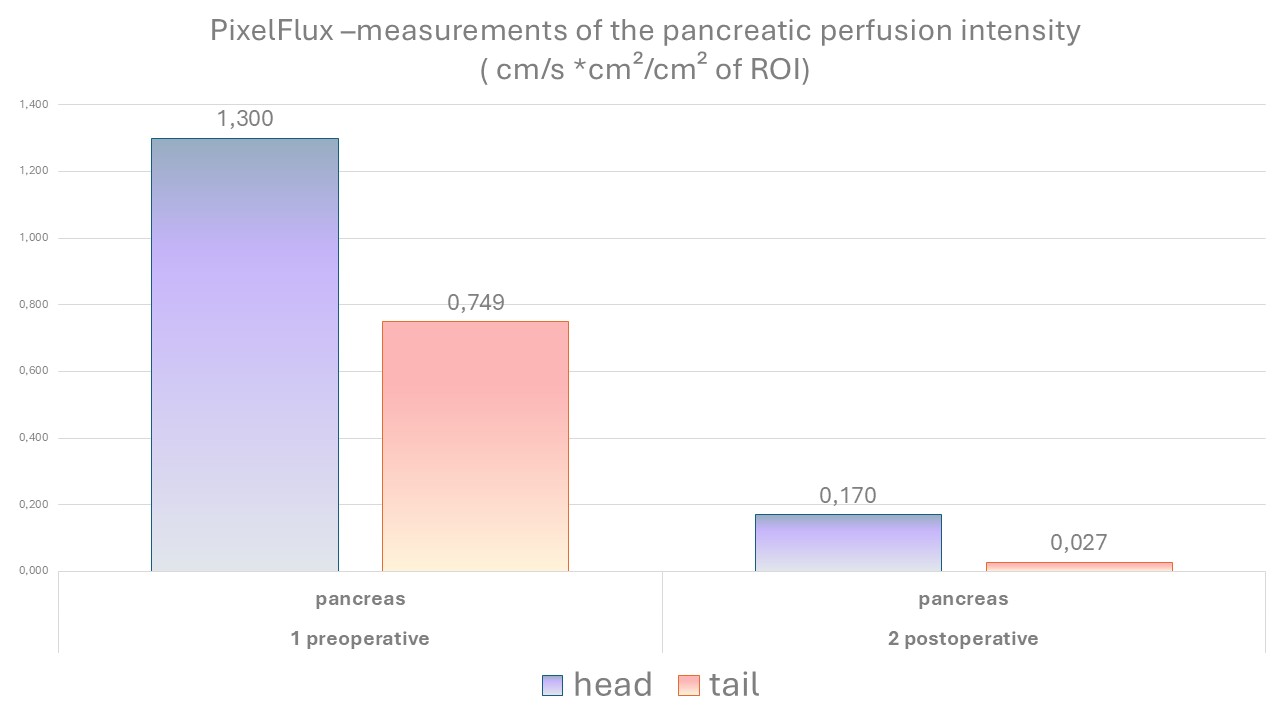
The PixelFlux measurement can quantify the extent of this congestion and also allow a comparison to the profound improvement with a complete resolution of this congestion after the decompression of the splenic vein. Obviously, the congestion of the pancreas was an effect of the involvement of the pancreas into the collateral pathway of the congested splenic vein.
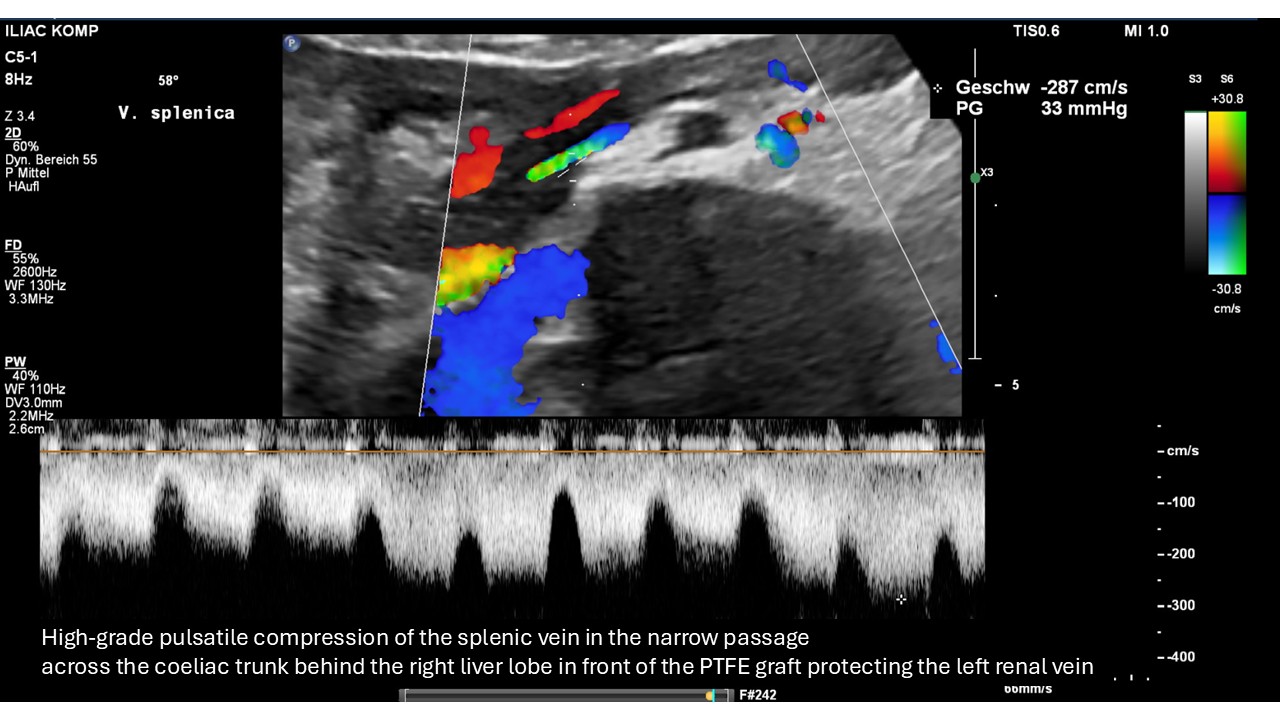
Strong flow acceleration within the splenic vein as a sign of its severe compression by the coeliac trunk (small round structure in the upper Centre of the image). The pulsatile nature of the flow acceleration is the proof that an artery-here the coeliac trunk-is the compressing structure.

Close-up view of the compression of the splenic vein the coeliac trunk.

Ultrasound B-mode image demonstrating the compression of the splenic vein with the surrounding structures which narrow the space for the splenic vein thus preparing its compression.

Spatial relationship of the PTFE graft protecting the formerly compressed left renal vein and the splenic vein showing that graft itself is not compressing the splenic vein.

After the surgical decompression of the splenic vein the flow velocity drops to the half of the preoperative values demonstrating the significant reduction of the

Detailed view of the now apparently vessel-free pancreatic tail after the are decompression of the splenic vein rendering the collateral pathway via the pancreas unnecessary.