- New stuff to read and discuss
- What patients say
- Clinic / online appointments
- Why the diagnosis of a psychosomatic illness is often a misdiagnosis
- Vascular Compression Syndromes
- Do you have questions?
- Checklist vascular compression syndromes
- Description of your symptoms
- Researchers from the Mayo Clinic confirm my concept of the Midline Congestion Syndrome
- Explanation of gender-specific differences in the clinical symptoms of abdominal vascular compression syndromes: varicocele and penile/testicular pain – their main manifestation in men.
- Varicocoele is predominantly caused by left renal vein compression
- Musculoskeletal pecularities of female puberty
- Lordosis /Swayback- Origin of many abdominal compression syndromes
- Bending of a straight vein compels its narrowing
- The lordogenetic midline congestion syndrome
- Neurological consequences of the midline congestion syndrome
- Successful treatment of a teenage girl who was unable to eat due to extreme postprandial pain and unable to walk due to spasticity in her left leg
- Severe ataxia in a young woman with severe spinal congestion – complete resolution after decompression of the left renal vein
- All compression syndromes are one: the spectrum of lordogenetic compressions
- Nutcracker-Syndrome is a misnomer! Lordogenetic left renal vein compression is a more appropriate name!
- May-Thurner-constellation (May-Thurner-syndrome, Cockett’s syndrome)
- Midline (congestion) syndrome
- Pelvic congestion syndrome
- Celiac Trunk Compression / Dunbar syndrome / MALS / Arcuate ligament syndrome
- Wilkie-Syndrome / Superior-mesenteric-artery-syndrome
- Compression of the vena cava inferior
- Evlauation of vascular compressions with the PixelFlux-method
- Connective tissue disorders predispose to multiple compressions
- Postural tachycardia syndrome (POTS) – the hemodynamic consequence of vascular compression syndromes and loose connective tissue
- Restless legs-a little known symptom of abdominal vascular compression syndromes
- Pudendal neuralgia in vascular compression syndromes
- A new sonographic sign of severe orthostatic venous pooling
- Migraine and Multiple Sclerosis
- Hemodynamic effect on cerebral perfusion in patients with multiple localised vascular compression.
- Treatment of vascular compression syndromes
- Fatal errors in the treatment of vascular compression syndromes
- Risks of stents in venous compression syndromes
- Surgical treatment of abdominal compression syndromes: The significance of hypermobility‐related disorders
- Nutcracker and May-Thurner syndrome: Decompression by extra venous tube grafting and significance of hypermobility related disorders
- Our surgical treatment of vascular compressions
- Chronic regional pain syndrome (CRPS) caused by venous compression and mechanical irritation of the coeliac plexus
- Vascular compression syndromes and other disease mechanisms I recently detected
- Kaleidoscope of instructive cases
- Venous congestion of the spinal cord may be a potential contributor to the development of paraplegia in patients with spinal muscular atrophy type III (Kugelberg-Welander disease)
- Ultrasound Diagnostics
- A breakthrough in functional sonographic diagnostic – 4D-colour Doppler sonographic flow volume measurements
- 4D-volume flow measurements of jugular and mesenteric veins
- Inauguration of the global volumetric brain perfusion measurement-a gateway for understanding of neurological symptoms
- Ultrasound focused entirely on all of your symptoms
- Ultrasound vs. X-ray
- Vascular Malformations
- Profile
- Functional colour Doppler ultrasound – how I do it
- Perfusion Measurement – PixelFlux-method
- Research
- Publications
- Nutcracker and May-Thurner syndrome: Decompression by extra venous tube grafting and significance of hypermobility related disorders
- Papers authored by Th. Scholbach
- Publications
- Inauguration of measurements of the tissue pulsatility index in renal transplants
- From nutcracker phenomenon to midline congestion syndrome and its treatment with aspirin
- First sonographic tissue perfusion measurement in renal transplants
- First sonographic bowel wall perfusion measurement in Crohn disease
- First sonographic renal tissue perfuison measurement
- First sonographic measurement of renal perfusion loss in diabetes mellitus
- PixelFlux measurements of renal tissue perfusion
- Why I prefer not to publish in journals but in the Internet
- Vessel stretching in nephroptosis – an important driver of complaints
- Publications
- Expertise
- Bornavirus Infection
- Scientific cooperation
- Cookie Policy
- Data protection
- Cookie Policy (EU)
- Impressum
Patient with severe post-prandial hyperventilation and circulatory issues due to compression of the vena cava by the diaphragm and the down sliding liver
The patient is a 35-year-old female with a long history of postprandial issues. Among other symptoms, she was unable to eat sufficient amounts of food. Specifically, she avoided solid foods, which were less tolerated than fluids. One of the main symptoms was shortness of breath after a meal, which she felt was life-threatening, especially when she stood upright after eating, at which point she also experienced circulatory issues, such as dizziness and near fainting.
For over 10 years, conventional gastroenterological and cardiological diagnostics could not determine the cause of the problem.
However, functional colour Doppler ultrasound revealed that the problems were caused by compression of the inferior vena cava. The patient’s increased lumbar lordosis, resulting from a connective tissue disorder (hypermobile Ehlers-Danlos syndrome), pushed the inferior vena cava ventrally.
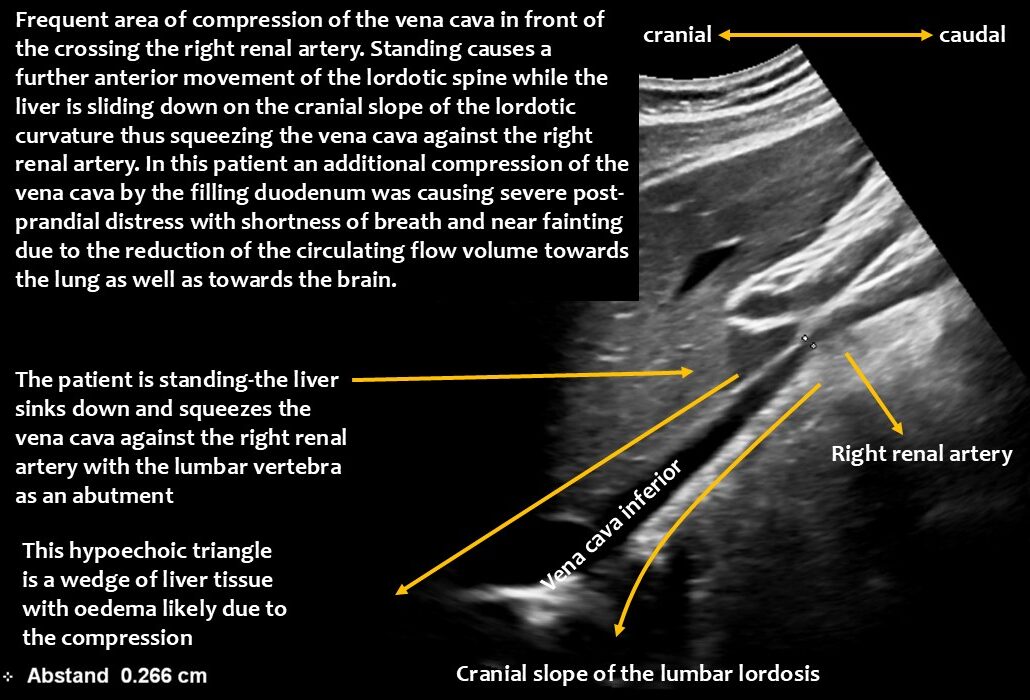
The upper lumbar vertebrae thus acted as a barrier against which the expanding duodenum pressed the vena cava. The situation was exacerbated by the duodenum not functioning properly, causing food to become lodged in the descending portion of the duodenum, directly in front of the inferior vena cava.
When the patient stood up, gravity pulled the liver downwards.
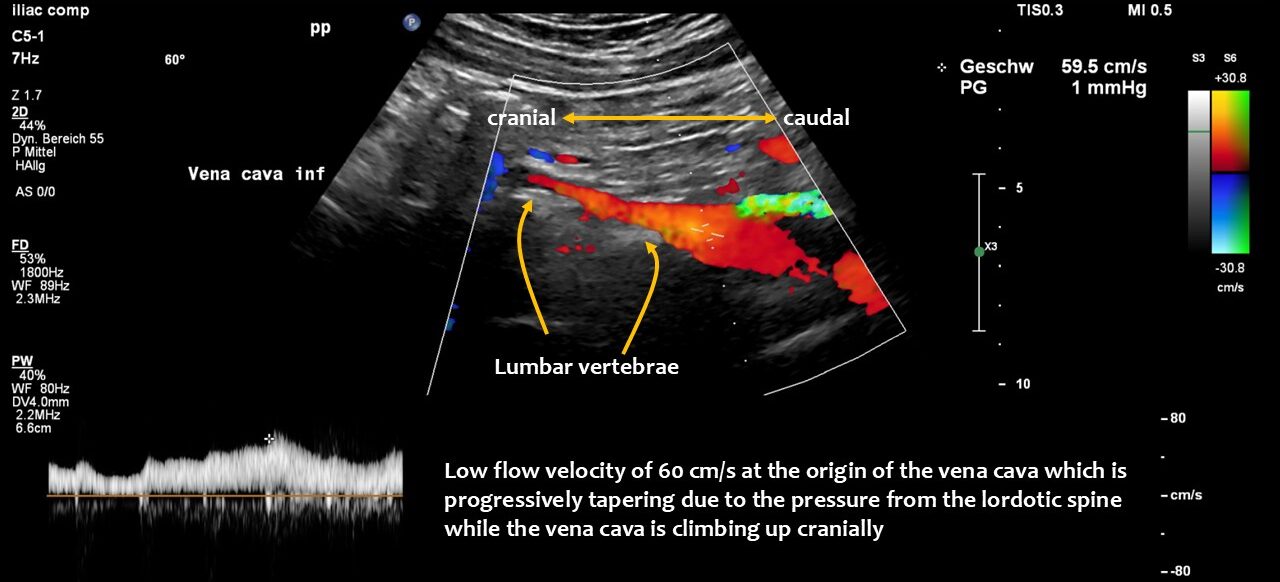
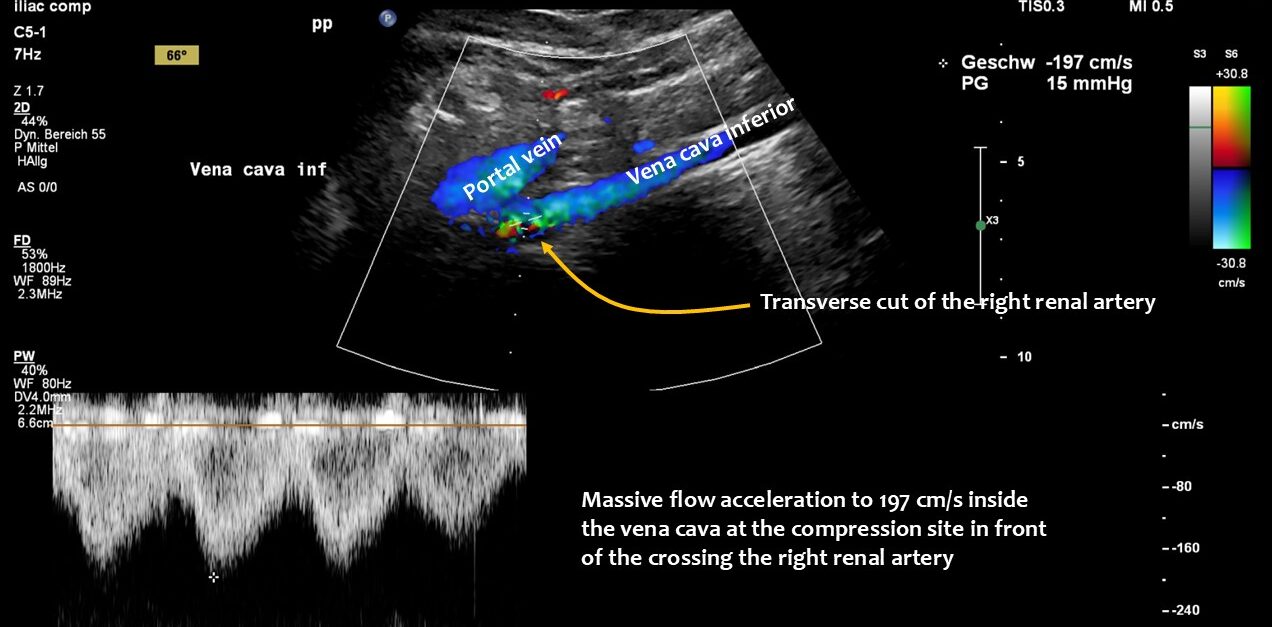
Due to the lax connective tissue, the liver was less fixed and thus developed orthostatic hepatoptosis, sliding down like a sled on a ramp — the cranial slope of the lumbar lordotic curvature — while standing. This compression was exacerbated by the perpendicular crossing of the right renal artery, which runs behind the vena cava and in front of the lumbar spine, acting as a bar and making the compression even more efficient.
Immediately after food was taken up, the stomach pumped it into the duodenum, which subsequently enlarged and compressed the vena cava.
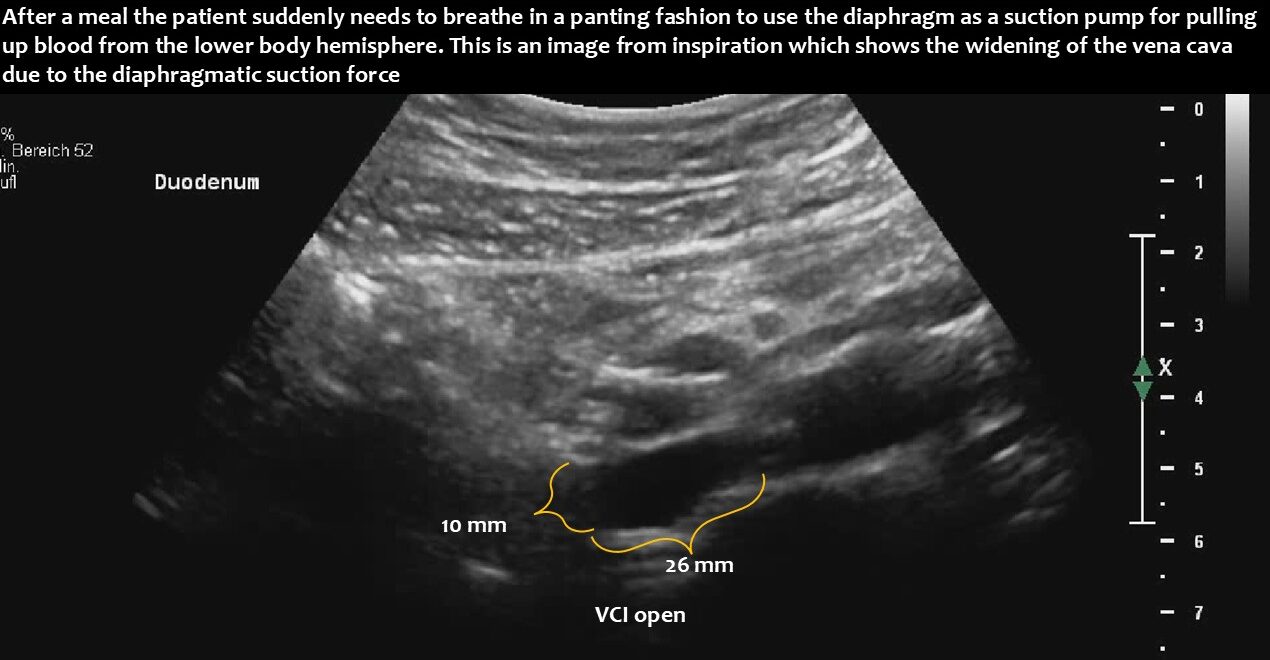
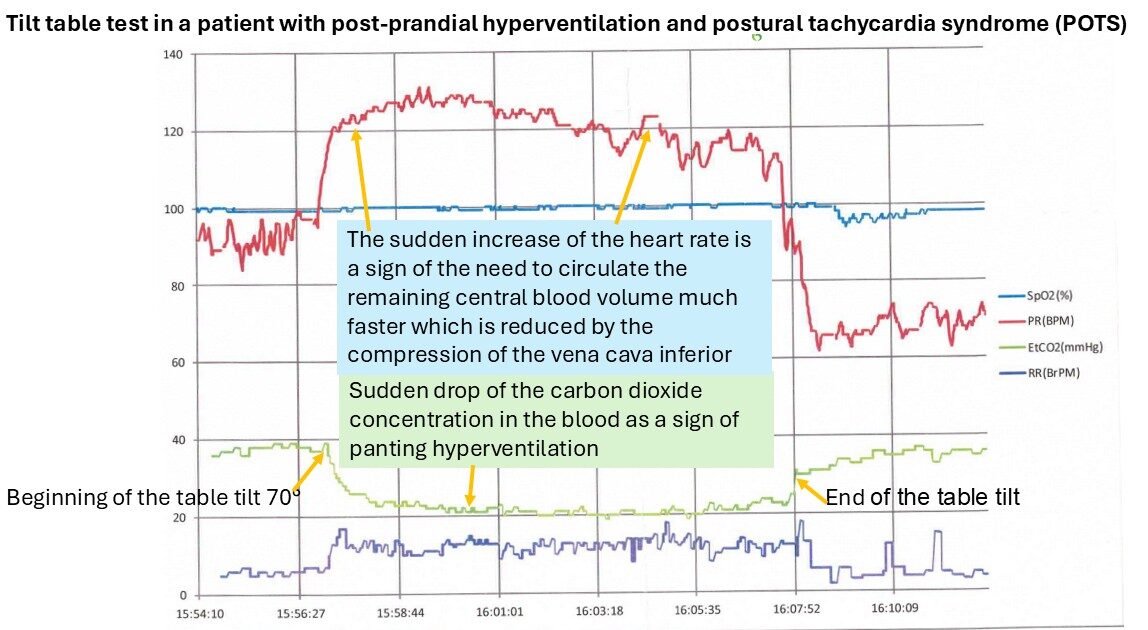
This suddenly interrupted or massively compromised the venous return from the lower body hemisphere. This led to a sudden drop in the circulating blood volume. Due to reduced lung perfusion as a consequence of the reduction in central flow volume, panting developed to enhance oxygenation of the remaining small blood volume. At the same time, the reduced blood flow to the brain, in combination with hypocapnia as a result of hyperventilation to fight imminent compromise of oxygenation, caused dizziness and a sensation of near fainting.
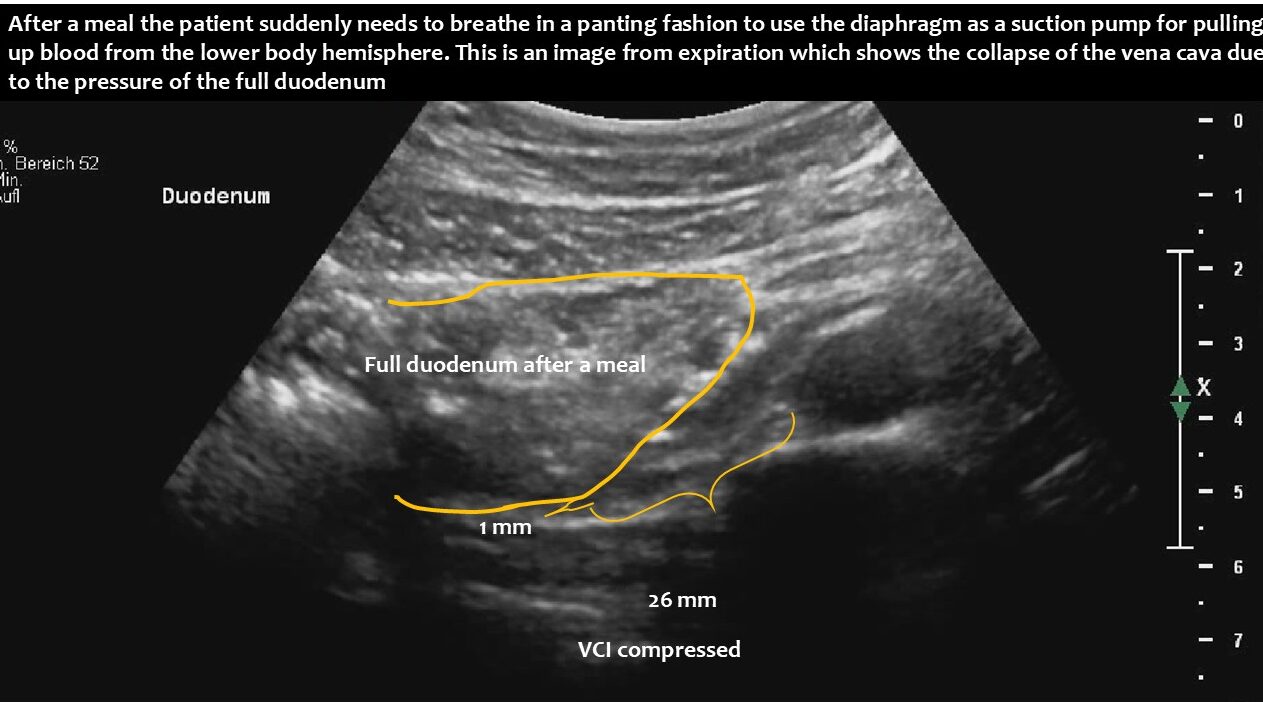
Functional ultrasound can demonstrate the entire pathophysiological chain, from underlying lordosis to postprandial duodenal enlargement and subsequent vena cava compression, especially when standing after eating.
The logical treatments are reducing the lordosis, training the back muscles, and eventually decompressing the vena cava by wrapping it in a PTFE shield.