- Neue Artikel
- Was Patienten sagen – Fortsetzung
- Praxis/ online Terminvergabe
- Warum die Diagnose einer psychosomatischen Erkrankung häufig eine Fehldiagnose ist
- Gefäßkompressionssyndrome
- Haben Sie Fragen?
- Checkliste Gefäßkompressionssyndrome
- Beschreibung Ihrer Symptome
- Erklärung der geschlechtsspezifischen Unterschiede bei den klinischen Symptomen von abdominalen vaskulären Kompressionssyndromen: Varikozele und Penis-/Hodenschmerzen – ihre Hauptmanifestation bei Männern.
- Die Varikozele wird überwiegend durch eine Kompression der linken Nierenvene verursacht
- Muskuloskelettale Besonderheiten der weiblichen Pubertät
- Lordose /Hohlkreuz – Ursache zahlreicher abdomineller Kompressionssyndrome
- Die Anhebung einer Vene erzwingt deren Kompression
- Truncuskompression bei Kindern
- Lordogenetisches Mittellinensyndrom
- Neurologische Folgen des Mittellinienstauungssyndroms
- Erfolgreiche Behandlung einer Teenagerin, die aufgrund extremer postprandialer Schmerzen nicht essen und aufgrund einer Spastik im linken Bein nicht gehen konnte.
- Schwere Ataxie bei einer jungen Frau mit schwerer venöser Rückenmarksstauung – vollständige Heilung nach Dekompression der linken Nierenvene
- Alle abdominalen Kompressionssyndrome liegen in der Lordose begründet
- Das „Nussknacker“-Syndrom ist eine Fehlbezeichnung
- May-Thurner-Konstellation /May-Thurner-Syndrom/Cockett’s syndrome/Vena iliaca-Kompressionssyndrom
- Mittelliniensyndrom (Stauung der Mittellinienorgane)
- Pelvines Kongestionssyndrom
- Truncus-coeliacus-Kompression / Dunbar-Syndrom / MALS / Ligamentum arcuatum-Syndrom
- Wilkie-Syndrom / Arteria-mesenterica-superior-Syndrom
- Kompression der Vena cava inferior
- Quantifizierung der Gefäßkompressionssyndrome mit der PixelFlux-Technik
- Bindegewebserkrankungen begünstigen kombinierte Kompressionssyndrome
- Posturales Tachykardiesyndrom (POTS) – die hämodynamische Folge von Gefäßkompressionssyndromen und lockerem Bindegewebe
- Unruhige Beine (restless legs) – Folge venöser Kompressionssyndrome
- Pudendusneuralgie bei vaskulären Kompressionssyndromen
- Ein neues sonographisches Zeichen für eine schwere orthostatische Beckenvenenstauung
- Migräne und Multiple Sklerose
- Behandlung von Kompressionssyndromen
- Fehler bei der Therapie von Gefäßkompressionssyndromen
- Embolisation – Irrweg bei venösen Kompressionssyndromen
- Risiken von Stents bei venösen Kompressionssyndromen
- Chirurgische Behandlung von abdominalen Kompressionssyndromen: Die Bedeutung der Bindegewebshypermobilität
- Nutcracker and May-Thurner syndrome: Decompression by extra venous tube grafting and significance of hypermobility related disorders
- Chronisches regionales Schmerzsyndrom (CRPS) verursacht durch Venenkompressionen und mechanische Reizung des Plexus coeliacus
- Vaskuläre Kompressionssyndrome, die ich kürzlich entdeckt habe
- Kaleidoskop lehrreicher Krankheitsverläufe
- Eine venöse Stauung im Rückenmark kann möglicherweise zur Entwicklung einer Querschnittslähmung bei Patienten mit spinaler Muskelatrophie beitragen.
- Ultraschalldiagnostik
- Leistungsspektrum
- Funktioneller Farbdoppler-Ultraschall – wie ich ihn verstehe
- Durchblutungsmessung – PixelFlux-Verfahren
- Forschung
- Publikationen
- Nutcracker and May-Thurner syndrome: Decompression by extra venous tube grafting and significance of hypermobility related disorders
- Veröffentlichungen von Th. Scholbach
- Eigene Publikationen
- Erstbeschreibung der Bestimmung des Gewebsperfusionsindexes in Nierentranplantaten
- Erstbeschreibung des Mittellininesyndroms – Aspirintherapie
- Erste sonografische Gewebsperfusionsmessung in Nierentransplantaten
- Erste sonografische Tumorperfusionmessung und Korrelation zur Tumoroxygenierung
- Erstmalige Darmwandperfusionsmessung bei M. Crohn
- Erstmalige sonografische Gewebsperfusionmessung der Nieren
- Erstmaliger Nachweis von Frühveränderungen der Nierenperfusion bei Diabetes mellitus
- PixelFluxmessung der Nierengewebsperfusion
- Publikationen
- Expertise
- Bornavirusinfektion
- Wissenschaftliche Zusammenarbeit
- Cookie-Richtlinie
- Hinweise zu medizinischen Erläuterungen
- Datenschutzerklärung
- Cookie Policy (EU)
- Impressum
Genitalschmerzen beim Sitzen – manchmal Pudendusneuralgie – hier lange unentdeckte subakute Bartholinitis bei hypermobilem Ehlers-Danlos-Syndrom und multiplen Kompressionssyndromen – Diagnose durch PixelFlux
Anamnese (Juni 2021)
Die Patientin leidet seit Januar 2020 an unerträglichen Schmerzen im Bereich der großen Schamlippe links, die im Sitzen unerträglich zunehmen, im Stehen von Stärke 8 auf Stärke 5 absinken und im Gehen etwa gleich stark empfunden werden. Diese Schmerzen sind immer vorhanden, außer nachts, und werden als eine innerliche Schwellung empfunden. Die Patientin hatte zwischenzeitlich Beschwerden im Sinn einer Cystitis, konnte auch morgens nur zögerlich die Harnblase entleeren. Nun ist die Miktion jedoch schmerzfrei, die Blasenentleerung unkompliziert möglich. Es besteht klinisch ein hypermobiles Ehlers-Danlos-Syndrom. Molekulargenetisch wurden alle anderen Formen des Ehlers-Danlos-Syndrom ausgeschlossen. Die Überdehnbarkeit des Bindegewebes kommt darin zum Ausdruck, dass die Patientin umstandslos den Daumen auf den ipsilateralen Radius pressen kann, im Stehen mit den Handflächen den Fußboden berühren kann, das Daumenzeichen und das Kleinfingerzeichen sind positiv.
Im Stehen hat die Patientin das Gefühl als würde etwas wie ein innerer Prolaps im Becken nach unten drängen.
Außerdem bestand ein nun reparierter Zwerchfellbruch.
Die Schmerzen im Bereich des Genitales wurden auch als Coccygodynie interpretiert. Eine Infiltration der Region mit einem Lokalanästhetikum brachte eine langfristige Linderung jedoch nicht ausreichend, um ungestört einer Berufstätigkeit bei sitzender Tätigkeit nachzugehen.
Außerdem bestehen in geringerem Maße links inguinal Leibschmerzen in einer Stärke von 3/10 und unter dem linken Rippenbogen Schmerzen in einer Stärke 2/10. Die Patientin berichtete auch über linksseitige Schmerzen im Bereich der Scapula und Schmerzen an der linken Halsseite, zum Teil mit Schluckbeschwerden einhergehend. Menstruationsschmerzen, Atemprobleme oder Schwellung der Beine werden verneint. Die Nahrungsaufnahme ist nicht beeinträchtigt. Erbrechen oder Durchfall bestehen nicht. Zahlreiche ärztliche Konsultationen erbrachten keinen befriedigenden Besserung ihrer Beschwerden. Seit 21. Mai besteht eine fortwährende vaginale Blutung, gynäkologischerseits wurde jedoch keine Therapie eingeleitet, der Untersuchungsbefund beim behandelnden Gynäkologen sei in Ordnung gewesen.
Klinischer Befund
Die Palpation und Auskultation des Abdomens sind unauffällig. Es besteht keine pathologische Resistenz. Bei der Palpation des Perineums lässt sich jedoch an der dorsalen Kommissur der Labien linksseitig ein heftiger Druckschmerz auslösen. Äußerlich besteht hier eine fragliche Rötung, keine Schwellung, keine Resistenz. Eine vaginale Sekretion besteht aktuell nicht.
Sonografischer Befund
Die Harnblase ist mäßig gefüllt, sonografisch unauffällig. Die Scheide ist nicht geschwollen aber von zahlreichen kleinen erweiterten Venen durchsetzt. Der Uterus ist kräftig, anteflektiert und zeigt erhebliche Zeichen einer pelvinen Kongestion mit schwammartig das Myometrium durchsetzenden erweiterten Venen, die insbesondere an der linken Zirkumferenz des Uterus stark ausgeprägt sind. Diese pelvine Kongestion erklärt die Schmerzen links inguinal. In der Vena iliaca interna links fließen leicht arteriell moduliert 667 ml/min nach kranial ab. Rechts sind 2 Venae iliacae internae darstellbar die gemeinsam 436 ml nach kranial ableiten. Die Perfusion links ist symmetrisch auf etwa das Doppelte angehoben. Die starke Perfusionssteigerung links erklärt sich aus der Entlastung der durch die Schwerkraft im Stehen zunehmend erweiterten Beckenvenen, nachdem sich die Patientin zur Untersuchung in Rückenlage begeben hat und damit der Einfluss der Schwerkraft auf die pelvine Kongestion nachlässt. Die Stauung links ist infolge der geringen Abflussbehinderung über die angeordnete Vena iliaca communis am Promontorium erklärbar (siehe unten).
Die Vena iliaca communis sinistra weist an der linken Flanke des Os sacrum eine Flussgeschwindigkeit von 35, an der Kreuzungsstelle mit der Arteria iliaca communis dextra ein Flussgeschwindigkeit von 89 cm/s auf. Eine echte Lumeneinengung ist an dieser Kreuzungsstelle jedoch nicht sichtbar. Die Flussbeschleunigung entsteht eher durch den bogenförmigen Verlauf über den Scheitelpunkt des Promontoriums hinweg.
In Rückenlage kann zu Untersuchungsbeginn eine auf 8 mm erweiterte Vena ovarica sinistra dargestellt werden. Nach mehrmaliger Umlagerung der Patientin und Einnahme einer stehenden Körperhaltung kollabiert das Gefäß jedoch bei Absinken der Baucheingeweide ins Becken. Insofern könnte phasenweise die pelvine Kongestion durch Bluteinstrom aus der linken Nierenvene über eine intermittierend retrograd durchblutete deutlich erweiterte Vena ovarica sinistra gespeist werden.
Die Vena cava ist nicht komprimiert.
Die ausgeprägte Lordose der Patientin hebt jedoch die Aorta soweit nach ventral, dass es zu einer fast vollständigen Kompression der linken Nierenvene am Übergang des Gefäßes über den bogenförmigen Abgang der Arteria renalis dextra kommt. Während im linken Anteil der Nierenvene die Flussgeschwindigkeit pulsatil moduliert bei 17 cm/s liegt finden sich an der Kompressionsstelle in Rückenlage Flussgeschwindigkeiten bis 262 cm/s!
In Rückenlage liegt das Flussvolumen in der Aorta abdominalis bei 3659 ml/min, die Flussgeschwindigkeit in der Aorta systolisch bei 98 cm/s.
Der Abgang des Truncus coeliacus ist durch das Ligamentum arcuatum umschrieben komprimiert was zu einer Flussbeschleunigung in Mittelposition des Zwerchfells auf 201 cm/s führt. In Inspiration verschwindet diese Kompression, die turbulente Strömung an der Kompressionsstelle lässt sich nicht mehr nachweisen und die Flussgeschwindigkeit fällt auf 108 cm/s ab. Damit besteht eine typische Konstellation eines Ligamentum arcuatum Syndroms, allerdings ohne relevante klinische Symptomatik, wenn man von der klinisch zu vermutenden Ösophagitis absieht.
Der gesamte Colonrahmen ist stark meteoristisch gebläht. Beim Absinken der Därme ins Becken im Stehen führt dies zu zunehmendem Druck auf die gestauten Beckenvenen und zu einer Zunahme der Beschwerden im Becken. In Rückenlage steht der obere Pol der linken Niere 19,5, der der rechten 17,4 cm kranial der Crista iliaca im Stehen verringert sich diese Distanz links auf 11,3, rechts auf 7,6 cm. Damit besteht eine deutliche Ptose beider Nieren, passend zum Ehlers-Danlos-Syndrom, vor allem rechts. Im Stehen kommt es phasenweise zu einer Entlastung der Kompression der linken Nierenvene, die jedoch nur kurzzeitig anhält. Es werden dann Flussgeschwindigkeiten an der Kompressionsstelle um 150 cm/s gemessen. Im Sitzen, welches für die Patientin besonders beschwerlich ist, steigt die Flussgeschwindigkeit durch zunehmende Kompression der linken Nierenvene wieder auf 263 cm/s an.
Die hämodynamische Relevanz der Nierenvenenkompression kommt in einer deutlich verminderten Volumenperfusion der linken Niere in der PixelFlux Messung zum Ausdruck. Diese Unterschied besteht vor allem im Liegen, die Perfusion der linken Niere liegt da bei etwa 40% der rechten Niere. Im Sitzen und im Stehen verursacht die ausgeprägte Ptose der rechten Niere, geringer auch links ausgeprägt, einen deutlichen Perfusionsabfall, insbesondere rechts und eine allgemeine Reduktion der Nierenperfusion. Dies trägt dazu bei, dass im Sitzen und im Stehen vermehrt Blut in die Beckenzirkulation eingespeist wird, wo es zur venösen Stauung bei trägt.

Parenchymperfusionsmessung beider Nieren mit der PixelFlux Technik Angabe der Perfusionsintensität in [cm/s * cm²/cm²] als mittlere Geschwindigkeit aller farbcodierten Pixel multipliziert mit der Fläche aller farbcodierten Pixel/die Fläche aller Pixel der Region of interest
Für einen Morbus Crohn finden sich weder im Rektum noch in anderen Darmabschnitten charakteristische sonografische Veränderungen.
Mit der PixelFlux Technik wird die Perfusion im Bereich des entzündlichen Infiltrats links perineal gemessen. Sie liegt bei einem Vielfachen der Perfusion des Gewebes rechts paravaginal. Aus sonografischer Sicht handelt es sich hier um eine Bartholinitis links. Eine entsprechende antibiotische Therapie wurde begonnen.

Parenchymperfusionsmessung Labia maiora mit der PixelFlux Technik Angabe der Perfusionsintensität in [cm/s * cm²/cm²] als mittlere Geschwindigkeit aller farbcodierten Pixel multipliziert mit der Fläche aller farbcodierten Pixel/die Fläche aller Pixel der Region of interest
Die differenzialdiagnostisch erwogene Nervus pudendus-Neuralgie links wird durch Untersuchung des Sitzbeins von medial und des Bereich des Alcock Kanals beleuchtet. Dabei lassen sich keine venösen Stauungszeichen im -Bereich des Nervus pudendus und des Alcock Kanals darstellen. Vielmehr liegt das Punktum maximum der Schmerzen deutlich medial des Nervus pudendus an der dorsalen Kommissur der großen Labien links.
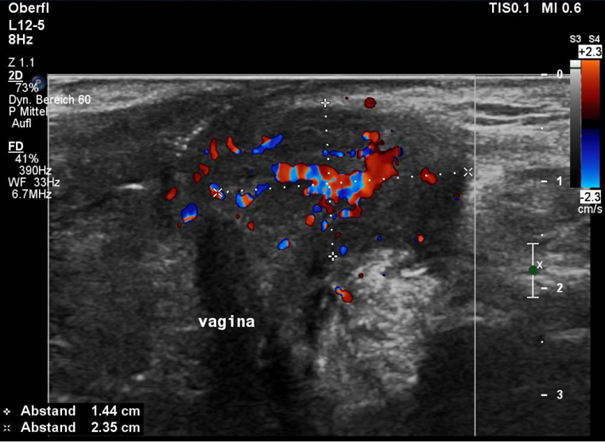
Transversaler Farbdoppler-Ultraschall der Vulva an der dorsalen Kommissur der großen Schamlippen. Auf der linken Seite findet sich eine gut abgrenzbare, hyperperfundierte entzündliche Infiltration an der Stelle der Bartholin’schen Drüse, genau dort, wo der Schmerz durch 1-Finger-Palpation lokalisiert wurde.
Diagnosen
- Nicht abszedierende Bartholinitis links-eine antibiotische Therapie mit 2 x 500 mg Cefuroxim wurde eingeleitet
- pelvine Kongestion bei Einspeisung von Nierenvenenblut (passager) über die Vena ovarica sinistra, vor allem aber infolge des klinischen
- hypermobilen Ehlers-Danlos-Syndroms
- geringgradige Flussbehinderung der linken Vena iliaca communis durch den bogenförmigen Verlauf des Gefäßes über das angehobene Promontorium
- klinisch fast inapparentes Ligamentum arcuatum Syndrom
- Massive lordogenetische Nierenvenenkompression links, durch Kollateralen unzureichend kompensiert
- ausgeprägte Ptose beider Nieren, rechts mehr als links
- hochgradige Perfusionsminderung vor allem der rechten Niere im Stehen mit konsekutiver Zunahme der Hyperperfusion der Beckenorgane
Transversaler Farbdoppler-Ultraschall der Vulva an der dorsalen Kommissur der großen Schamlippen. Auf der linken Seite findet sich eine gut abgrenzbare, hyperperfundierte entzündliche Infiltration an der Stelle der Bartholin’schen Drüse, genau dort, wo der Schmerz durch 1-Finger-Palpation lokalisiert wurde.