Detection of a new mechanism of abdominal pain – painful orthostatic small bowel congestion
I report here for the first time a painful orthostatic congestion of the small bowel in a patient with left renal vein and left common iliac vein compression.
Medical history
The 35-year-old female patient had been suffering from urgency and cystitic pain for many years. Shortly before the first examination, she developed genital pain, mainly in the clitoris, accompanied by labial swelling. The patient reported also on the mucous during defecation but no blood in the stools. The anus was not painful.
Sonographic findings
Quantitative functional colour Doppler sonography revealed a severe congestion of the external genitals mainly the clitoris and the introitus of the vagina and around the anus.
May–Thurner syndrome was identified as the underlying cause of the congestion. An increased lumbar lordosis pushed the ventral surface of the spine 9 mm from the inner lining of the abdominal wall, uplifting the promontory and squeezing the left common iliac vein against the crossing right common iliac artery.
The increased lordosis also resulted in severe compression of the left renal vein, contributing to pelvic congestion and genital pain by causing collateralisation of left renal venous blood via the left ovarian vein towards the pelvis. Despite there being no clinical signs of loose connective tissue — the Beighton score was 0/9 — the patient exhibited substantial orthostatic right-sided nephroptosis, with an orthostatic movement of the right kidney of 8.9 cm, whereas the left kidney sank by only 3.1 cm while standing.
Despite being advised otherwise, the patient opted for embolisation of the left internal iliac vein and stenting of the left common iliac vein, rather than decompression of both veins.
14 months later the patient developed periumbilical and epigastric pain. A coeliac trunk compression was ruled out. The epigastric pain was referred to the left renal vein compression. The patient then received a decompression of the left renal vein by wrapping the vein into an external tubular shield which completely resolved the congestion of the left kidney and pelvic congestion as well as severe genital pain .
However, the patient reported persistent pain in the left paraumbilical region, which changed when body posture was changed.
Posture dependent pain left to the umbilicus
The pain was located to the left of the umbilicus when standing. Here, increased perfusion of the small bowel was observed, which disappeared when the patient lay down. A substantial swelling of the jejunal wall to 7 mm in the area left of the umbilicus was eye-catching .
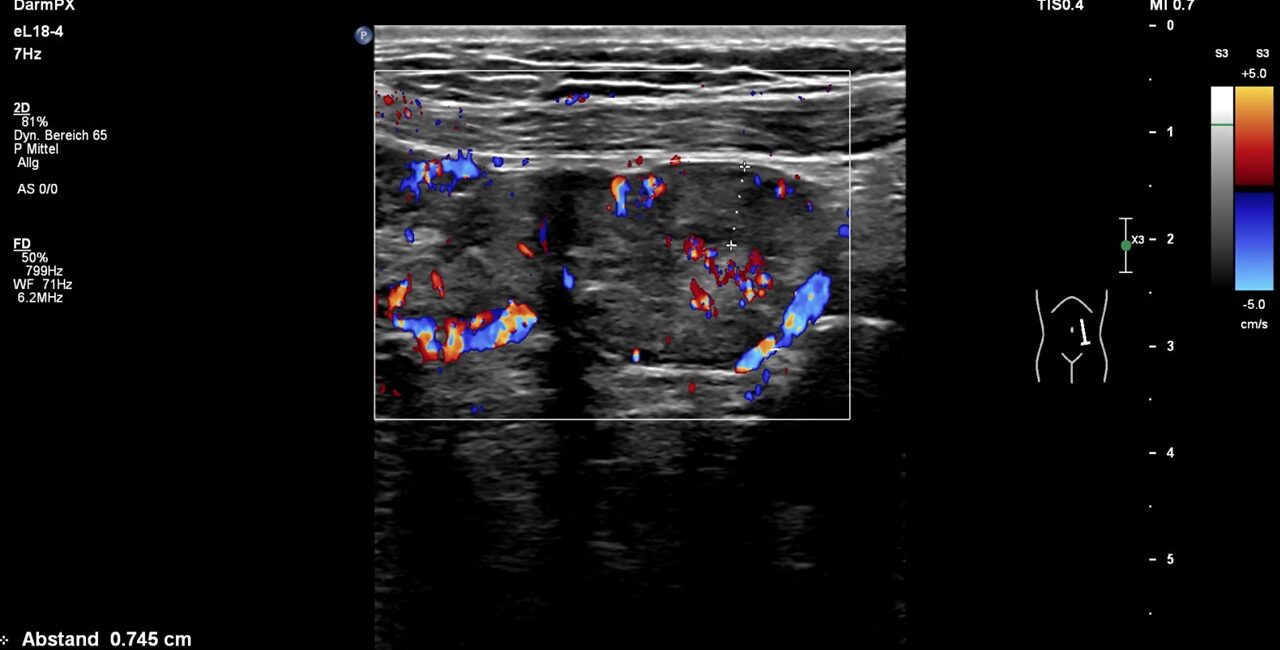
Massively swollen (7,5 mm, normal up to 2 mm) painful (palpation under sonographic guidance) jejunal loop with hyperperfusion
The thickened wall was significantly hyperperfused. Winding mesenteric veins could be seen running towards the thickened bowel loop.
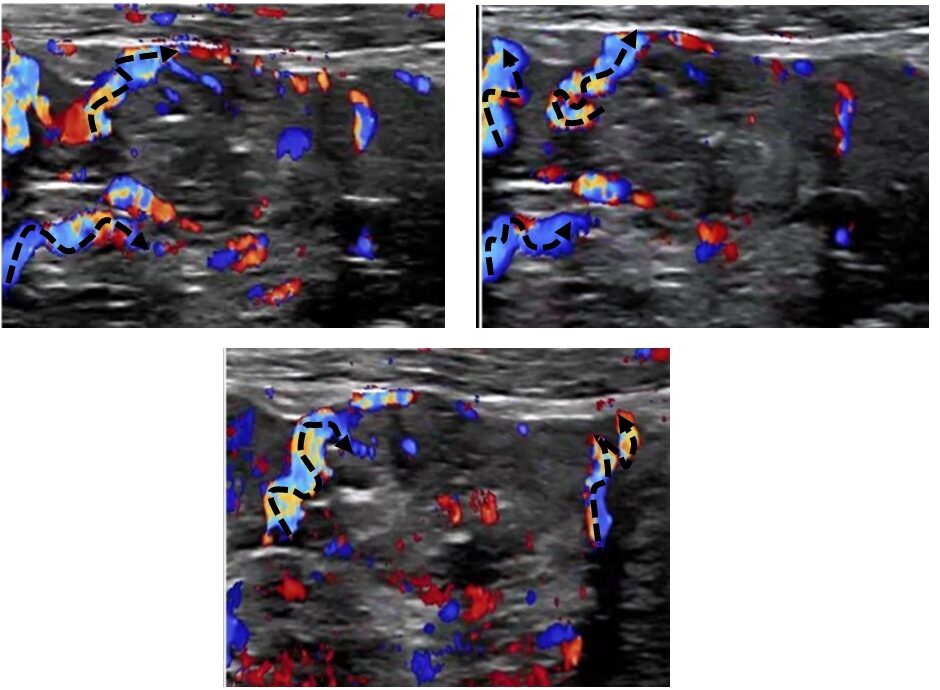
Winding mesentric veins (dashed arrows) running towards a thickend painful jejunal loop
While changing body posture , the perfusion of the hyperperfused small bowel changed rapidly. To investigate this further, the venous and arterial perfusion of the small bowel was examined. There was no compromise to the superior mesenteric artery.
The mesenteric vein showed no compression and the flow in the portal and hepatic veins up to the confluence with the inferior vena cava is normal. Portal flow was hepatopetal, slightly undulating, which is normal.
Mesenteric vein flow volume measurements
The flow volume quantification however led to an impressive finding. The superior mesenteric venous flow volume dropped from 889 mL/min while lying horizontally to 444 mL/min while standing.
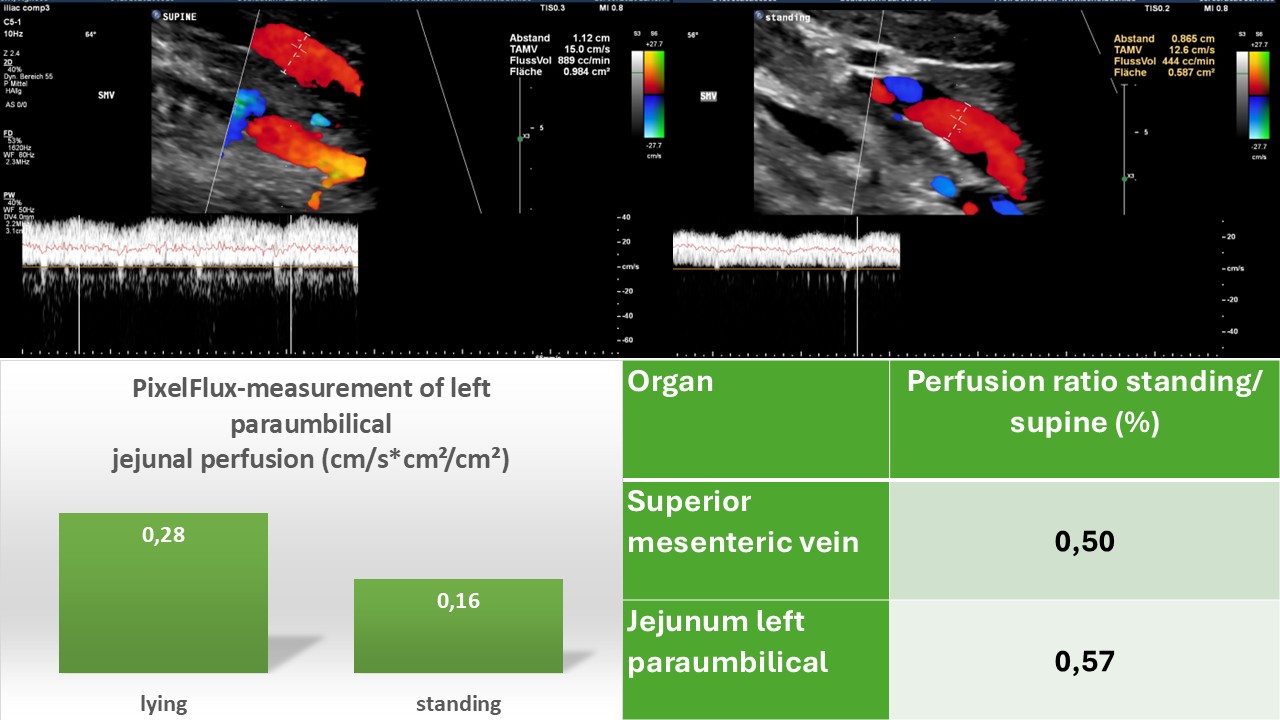
Posture dependent flow volume changes in the superior mesentric vein and synchronously with similar extent in the jejunal wall
Posture-dependent hyperperfusion and swelling of the small bowel, accompanied by pain was felt only when standing to the left of the umbilicus. This was evidently due to orthostatic congestion of the small bowel while standing since an outflow obstruction could be ruled out .
The tortuous distension of the small jejunal branches of the first jejunal vein [1] resulting in a pronounced venous marking of the thickened bowel wall was likely due to soft venous walls, distending under the recurrent frequent pressure changes during daily life while changing body posture from lying to standing or sitting. This transformed these veins which had all the characteristics of varicose veins (tortuous course, changing diameter, bud- like protrusions).
In contrast to inflammatory hyperperfusion, where only tiny veins inside the bowel wall are distended, here, larger veins in the mesentery also showed distension and winding, indicating gravitational congestion, comparable to varicose veins in the legs in some patients .
The ratio of the change in mesenteric venous flow volume in response to posture is reflected by a synchronous reduction in jejunal perfusion in the left paraumbilical region. Since a clear synchronicity was observed between the changing intensity of pain, the change in posture and the change in jejunal perfusion on the left side of the umbilicus, the exact location of the pain, it is concluded that swelling of the jejunum wall is a result of bowel congestion.
An obvious differential diagnosis of a hyperperfused and thickened jejunal wall would be a chronic inflammatory bowel disease. However, while inflammation is characterised by numerical increase of multiple small vessels restricted to the mucosa or submucosa of the small bowel, this patient exhibited in addition large winding vessels within the mesentery , indicating distension of the veins inside the mesentery and bowel wall due to orthostatic distension caused by congestion.
The PixelFlux perfusion measurement of the jejunal wall revealed a decrease of the perfusion by 43% after assuming an upright posture (see image above). The extent of the perfusion change of the jejunal wall was in the same range as the change of the flow volume of the superior mesenteric vein.
Discussion
To the best of my knowledge, a mechanism involving significant changes in the volume of blood flowing through the mesenteric vein, resulting in painful swelling and posture-dependent pain within a jejunal loop, has not yet been described.
For a long time however abdominal pain in patient with postural tachycardia is regarded a comorbidity for which no explanation has been offered so far [2, 3]. Patients with hypermobile Ehlers-Danlos syndrome suffer from widespread pain including up to 62% within the abdomen[4, 5] . They often develop a postural tachycardia[6]. A connection, however, between these conditions which according to my own experience are frequently associated with vascular compressions has not been described.
However, orthostatic congestion is a well-known consequence of vascular compression syndromes. Its main manifestations are orthostatic congestion of the genitals and legs. In these patients, compression of the left renal vein forces large volumes of blood from the left renal vein into the pelvic circulation via the left gonadal vein , where it is trapped by compression of the left common iliac vein. When the patient stands up, gravity comes into play, holding the blood within the pelvis by the joint effect of obstructed venous return and gravity, which forces the blood into the lower parts of the body.
This is the first case where a similar mechanism is observed within the jejunum.
The patient’s pain localisation is left to the umbilicus but without strict borders and somewhat fluctuating localisation since the small bowel is movable due to the variable position of the mesentery.
The jejunal trunk and the first jejunal vein typically cross the superior mesenteric artery dorsally to the left of the umbilicus [1]. This may contribute to their compression during change of body posture. While standing lumbar lordosis increases which may contribute to the compression of these veins against the superior mesenteric artery.
It may be worthwhile ruling out postural intestinal congestion in patients with connective tissue disorders, such as various types of EDS or postural tachycardia, who suffer from unexplained abdominal pain which so far frequently is attributed to psychological issues.
Literature
- Desai, G. and P.K. Wagle, First jejunal vein, jejunal trunk, and pancreatico-duodenectomy: resolving the literature conundrum. Langenbecks Arch Surg, 2023. 408(1): p. 104.
- Alexander, M.E., Orthostasis, the autonomic nervous system, and abdominal pain in children: is there a relation between postural orthostatic tachycardia and recurrent abdominal pain? J Pediatr Gastroenterol Nutr, 2008. 47(5): p. 696–700.
- Fortunato, J.E., et al., Effect of fludrocortisone acetate on chronic unexplained nausea and abdominal pain in children with orthostatic intolerance. J Pediatr Gastroenterol Nutr, 2014. 59(1): p. 39–43.
- Voermans, N.C., et al., Pain in ehlers-danlos syndrome is common, severe, and associated with functional impairment. J Pain Symptom Manage, 2010. 40(3): p. 370–8.
- Fikree, A., et al., Gastrointestinal involvement in the Ehlers-Danlos syndromes. Am J Med Genet C Semin Med Genet, 2017. 175(1): p. 181–187.
- Kucharik, A.H. and C. Chang, The Relationship Between Hypermobile Ehlers-Danlos Syndrome (hEDS), Postural Orthostatic Tachycardia Syndrome (POTS), and Mast Cell Activation Syndrome (MCAS). Clin Rev Allergy Immunol, 2020. 58(3): p. 273–297.