- El consultorio / Programación de citas en línea
- Compresiones vasculares
- ¿Tiene alguna pregunta?
- Lista de control Síndromes de compresión vascular
- Lordosis – Causa de numerosos síndromes de compresión abdominal
- Síndrome de May-Thurner/ síndrome de Cockett/ síndrome de compresión de la vena ilíaca
- Síndrome de la línea media (síndrome de congestión de la línea media)
- Síndrome de congestión pélvica (congestión de los órganos pélvicos)
- Compresión del tronco celíaco /síndrome de Dunbar/ síndrome de AMS/ síndrome del ligamento arcuato
- Síndrome de Wilkie/ síndrome de la arteria mesentérica superior
- Compresión de la vena cava inferior
- Neuralgia púdica en los síndromes de compresión vascular
- Tratamiento de los síndromes de compresión vascular
- Síndromes de compresión vascular que he detectado recientemente
- Kaleidoscope of instructive cases
- Servicios
- Ultrasonido Doppler color funcional – lo que entiendo por esto
- Medición de la circulación sanguínea – Método PixelFlux
- Investigación
- Perfil
- Infección por virus Borna
- Colaboración científica
- Cookie Policy
- Cookie Policy (EU)
Abdominal pain and weight loss due to habitual compression of the superior mesenteric vein-a new member in the family of midline compression syndromes
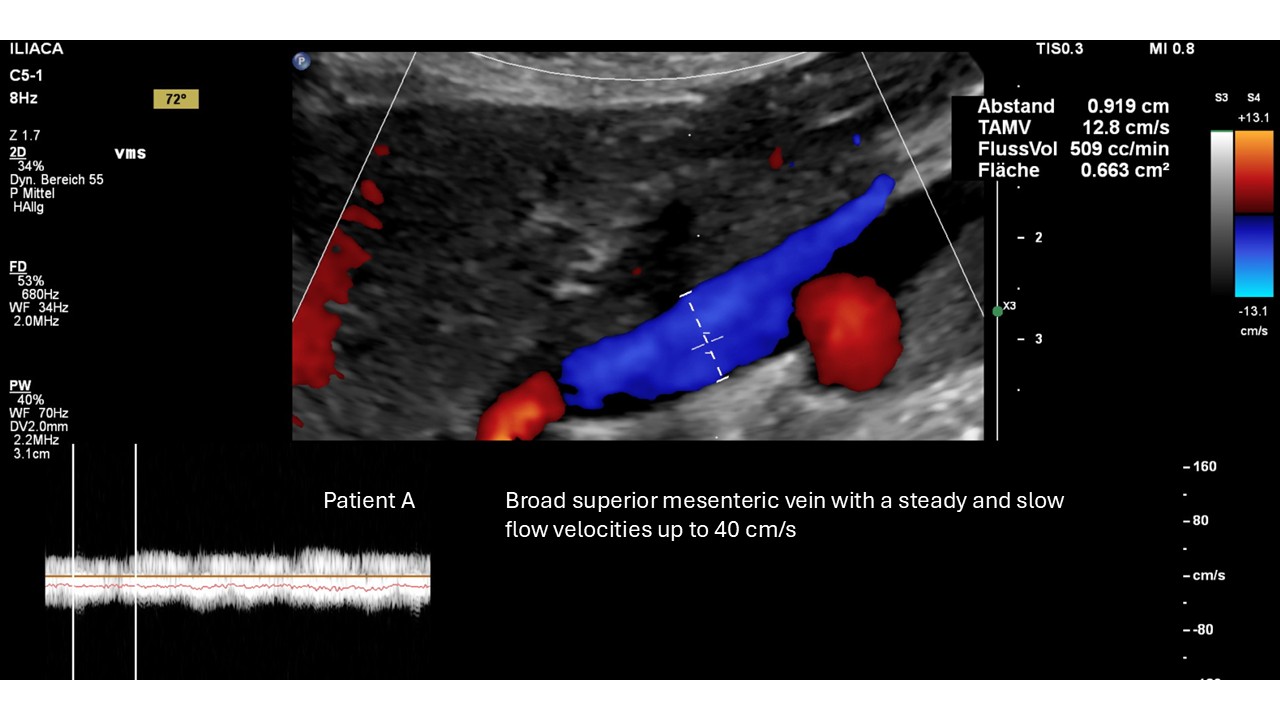
I describe below a previously unknown venous compression syndrome of the superior mesenteric vein by the hepatic artery at its confluence with the splenic vein characterized by post-prandially unbearable abdominal pain, post-prandial distension of the abdomen mainly in the right upper abdomen, and the inability to eat sufficiently leading to weight loss to cachexia .
Case presentation
The four patients presented here, are three women aged 41 (A), 25 (B), 22 (D), a young man (15 years).
The patients experienced the following main symptoms, which significantly overlapped:
Patient A experienced a weight loss of 12 kg within 12 months. Feeling full after eating for about 15 minutes, followed by bloating and loud, stormy bowel movements audible externally. She discharged bloody stools despite an unremarkable colonoscopy and suffered from recurrent diarrhea as well as change in bowel habits from constipation to diarrhea. Slow intestinal transport caused severe pain in the right flank. Due to pain and nausea, the patient was unable to eat and was on the brink of parenteral nutrition with a BMI of 14. The patient also experienced recurrent thrombosis of the anal canal, gastroparesis, incomplete paraparesis, and numbness of the anus and rectal canal.
Patient B has experienced frequent abdominal pain since early childhood, with increasing intensity. She required total parenteral nutrition and percutaneous gastrostomy. She experienced unbearable pain when fed via the gastrostomy. Her postprandial pain was localized in the right hypochondrium. She lost 30 kg in the last six months. In addition, severe nausea and frequent vomiting, loss of appetite or hunger, extreme constipation, burping, early satiety, intestinal bleeding, bloating, dizziness, tachycardia, shortness of breath, and episodes of dyspnea were reported . She had to use a wheelchair due to instability in her knee joints.
Patient C has suffered from chronic, postprandial abdominal pain since very early childhood. He started preferring mashed food at an early school age. He developed increasing weakness due to malnourishment from his inability to consume sufficient food. The patient experiences postprandial pain in the upper midline abdomen at a level of 8/10, starting three minutes after the first bite. He suffers from chronic headaches and vertigo that worsen when he stands or sits. He is unable to stand for a few minutes and requires parenteral nutrition for 60% of his daily calories.
Sonographic examination showed duodenal motor or dysfunction despite active gastric contractions. This resulted in cessation of intestinal transport in the descending portion of the duodenum.
Patient D suffered from unbearable post-prandial pain in the right hypochondrium, daily diarrhoea, inability to take up sufficient amount of food, headaches, menstrual pain. She experienced a weight loss of 9 kg within 24 months.
Her sonographic examination revealed signs of small bowel dysfunction including significant meteorism, disturbed peristalsis, distension of the descending portion of the duodenum, retroperistalsis, immediate gas formation in the duodenum after food contact, a feeling of disturbed food transport without evidence of duodenal compression, and severe constipation.
The patients suffered from other abdominal vascular compression syndromes:
| Patient A (41y) female | Patient B (25y) female | Patient C (15y) male | Patient D (23y) female |
| BMI 15.06 | BMI 14.13 | BMI 12.73 | BMI 19,10 |
| -12 kg | -30 kg | -9 kg | |
| Common diagnoses in all 4 patients:
Massive lordosis of the lumbar spine nearly touching the abdominal wall Pelvic congestion Left common iliac vein compression (“May Thurner syndrome”) Left renal vein compression (“Nutcracker syndrome”) Cachexia (BMI < 20) Simultaneous compression of the splenic and the superior mesenteric vein (at the confluence of both veins in patients A, C and D and a separate locations in patient B Massive additional orthostatic venous pooling causing difficulties standing (postural tachycardia syndrome, increasing pelvic pain) Severely reduced depth of the abdominal cavity due to an increased lordosis in combination with a flat thorax
Other diagnoses occurring not in all 4 patients
Loose connective tissue- clinical hypermobile Ehlers-Danlos syndrome A, B, C Compression of the jugular vein B Compression of the vena cava A,B Tronc réno-rachidièn A, C, Spinal congestion B, C Median arcuate ligament syndrome B, D Orthostatic nephroptosis A, B, D Peristaltic weakness of the duodenum C the the Bornavirus infection C Compression of the antrum pylori and subsequent delayed gastric emptying A Venous congestion of the liver with hepatomegaly A Hepatoptosis and enteroptosis/Gastroptosis A Prompt massive gas formation in the duodenum and stomach postprandially with reflux from the duodenum into the stomach A
|
|||
Colour Doppler sonographic imaging
Abdominal vascular compression syndromes are caused by the narrowing of the abdominal cavity due to increased lumbar lordosis and a flat thorax with reduced sagittal width at the upper and lower aperture. The increased lumbar lordosis is pushing the organs ventrally thus compressing for instance the left renal vein and the left common iliac vein. In addition, the shallow abdominal cavity, which is a consequence of a reduced anterior-posterior diameter of the lower thoracic aperture squeezes the bowel against the uplifted veins thus contributing to the compression depending on the filling of the bowel.
One way to measure this is by determining the minimum distance between the inner lining of the abdominal wall and the highest apex of the lordotic curvature.

Extreme narrowing of the abdominal cavity due to the lordotic uplifting of the lumbar spine and a flat thorax reducing the minimum distance at the level of the intervertebral disc L3/L4 to less than 6 mm only!
Regarding the development of gastrointestinal symptoms, it is important to note that the small intestines, which lie ventral to the spine and compete with the patient’s soft veins for space in the midline of the abdominal cavity, require a minimum space of 20-25 mm during peristalsis. This explains why these patients experience cramping pain in the mid and lower abdomen, which radiates towards the pelvis, about 30 minutes after beginning a meal. Assuming normal peristaltic activity, this is the time when food arrives in the lower abdomen. Then, the filled jejunum and ileum enlarge to a transverse diameter of 20-25 mm, which is obviously greater than the minimum distance found in the four patients presented here. The measurements were taken while the patients were lying supine, and they would probably decrease further while standing due to increased lumbar lordosis.
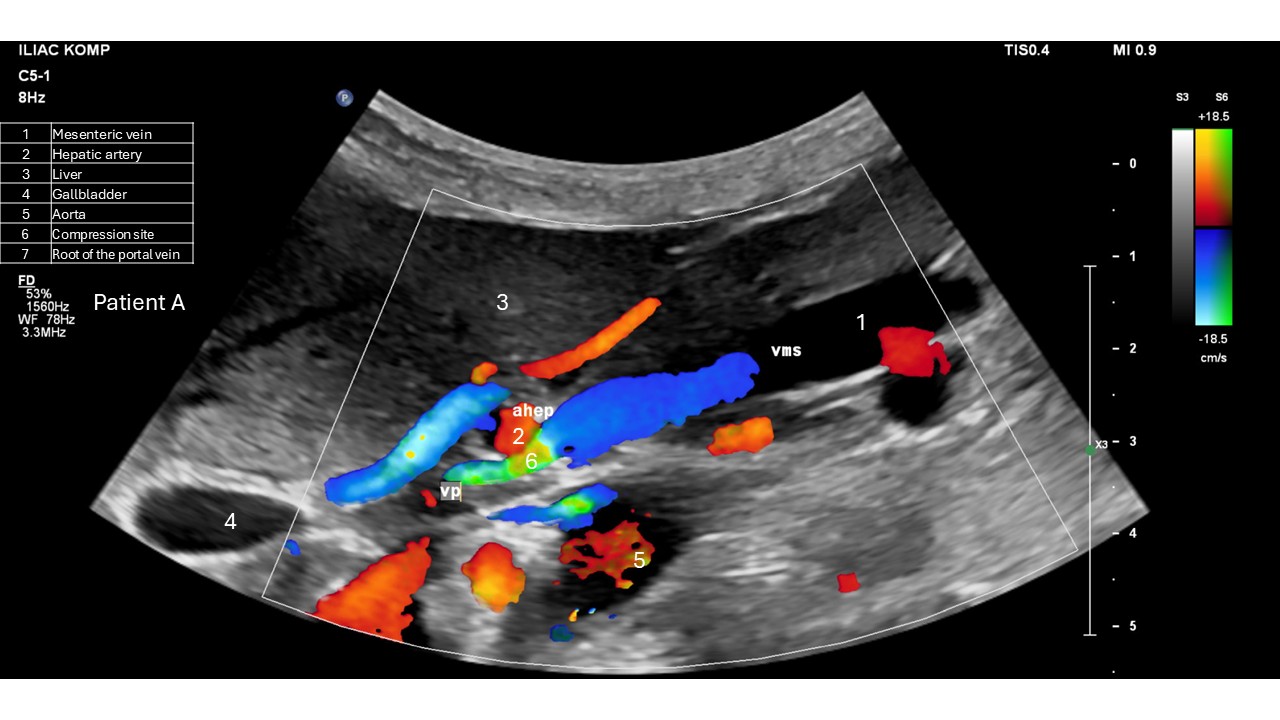
The compression of the superior mesenteric vein is easily depicted with the so-called variants mode highlighting the turbulence is produced by the vessel is narrowing in yellow/green.
| Patient | Minimal distance between the inner lining of the abdominal wall and the ventral surface of the spine (mm) |
| A | 15 |
| B | 8 |
| C | 6 |
| D | 10 |
The compression of the superior mesenteric vein is easily depicted vein using a colour scale in the variance mode. Then turbulences due to the narrowing of the vessels are highlighted in green/yellow enhancing their visibility.




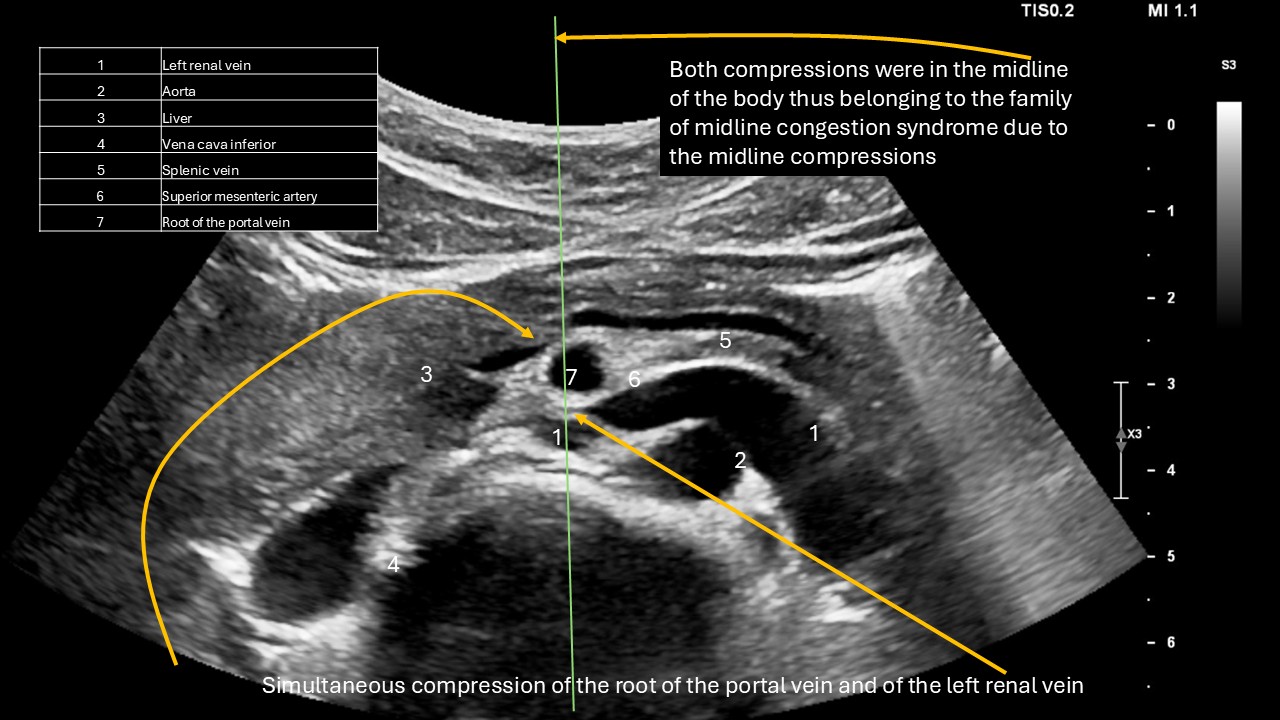
 Since the affected patient’s suffered substantial weight loss is often possible to demonstrate the compression of the root of the portal vein at the mouth of the superior mesenteric vein in conventional B-mode ultrasound images:
Since the affected patient’s suffered substantial weight loss is often possible to demonstrate the compression of the root of the portal vein at the mouth of the superior mesenteric vein in conventional B-mode ultrasound images:

Here is a comparison of the B-mode and colour Doppler sonographic imaging of the same patient:
 The substantial flow acceleration demonstrated here with the spectral analyses of the flow pattern is the core of the diagnosis:
The substantial flow acceleration demonstrated here with the spectral analyses of the flow pattern is the core of the diagnosis:


The superior mesenteric vein compression is exactly in the midline of the body as left renal vein compression, left iliac vein compression and coeliac trunk compression. The new entity thus is a member of the family of the midline compression syndromes which result basically from a increased lumbar lordosis:
Postural tachycardia due to a massive volume shift toward the lower body occurred in all patients, causing an inability to stand and signs of postural tachycardia syndrome.
The reduced return of venous blood towards the heart while standing is usually due to a combination of compression of the left common iliac vein or vena cava inferior reducing the return of blood towards the heart and the laxness of the veins which massively dilate while standing under the pressure of gravitation.
The following video shows the distension of the vein in orthostasis:
Quantitative color Doppler sonography was used to evaluate the extent of this venous pooling, which was observed as a reduction in left ventricular filling while standing compared to a horizontal posture.
| Patient | Trunk position | Aortic flow volume (ml/min) | Heart rate (1/min) v sys (cm/s) | Aortic systolic flow velocity (cm/s) (cm/s) | Abdominal proportion of left ventricular stroke volume (ml) |
| A | horizontal | 2736 | 59 | 92 | 46 |
| A | upright | 2192 | 61 | 56 | 36 |
| A | orthostatic difference (%) | -20% | 3% | -39% | -23% |
| B | horizontal | 2347 | 84 | 115 | 28 |
| B | upright | 2887 | 85 | 103 | 34 |
| B | orthostatic difference (%) | 23% | 1% | -10% | 22% |
| C | horizontal | 6430 | 69 | 172 | 93 |
| C | upright | 2877 | 92 | 97 | 31 |
| C | orthostatic difference (%) | -55% | 33% | -44% | -66% |
| D | horizontal | 5305 | 89 | 139 | 93 |
| D | upright | 2478 | 103 | 79 | 31 |
| D | orthostatic difference (%) | -53% | 16% | -43% | -60% |
A normal orthostatic perfusion drop is less than 8%. For affected patients, however, it ranged between 22 and 66%.
This caused severe cerebral and circulatory symptoms when upright, whether sitting or standing. Patients could not sit or stand for even a few minutes without becoming dizzy or nearly fainting. Patient C was so severely affected that he lost his ability to remember, so he could not write simple texts. He was constantly on the verge of losing consciousness and had to lie down constantly. Impressively, after decompressing the left renal vein and the left common iliac vein, he could walk up to 10 km a day, although he still could not stand for long periods of time, despite reducing his left ventricular filling loss to 30%. However, he could memorize again, sit upright for longer periods, and interact with his family members.
However, all four patients suffered from congestion of the small intestines due to compression of the mesenteric vein at its unification with the splenic vein. Four-dimensional PixelFlux volume flow measurements of the mesenteric vein clearly demonstrate the reduced flow volume of the vein at the outset and the insufficient increase of bowel perfusion due to the outflow obstruction from the small bowel:

The congestion of the small bowel may contribute to its motor dysfunction is demonstrated here on the duodenum of a patient:
The distending duodenum can contribute to an additional compression of the superior mesenteric vein peripheral to the compression by the hepatic artery as demonstrated in this patient:
Moreover, the reduced peristalsis and back and forward movement of the intestinal content may contribute to bacterial overgrowth and massive sudden post-prandial gas production which further requires space in the already restricted abdominal cavity. In this video the compression of the vena cava is demonstrated by the gas filling of the duodenum in a patient with superior mesenteric vein compression:
Orthostatic nephroptosis was determined sonographically by measuring the distance between the upper or lower pole of the kidney and the ipsilateral iliac crest.
Two of the four patients (A, B) had nephroptosis of the right kidney, which could be explained by simultaneous hepatoptosis.
| Patient | left kidney | right kidney | Body length (cm) | Percentage left ptosis | Percentage right ptosis |
| A | 3,6 | 9,3 | 167 | 2% | 6% |
| B | 3,1 | 12,3 | 164 | 2% | 8% |
| C | 4,5 | 3,6 | 188 | 2% | 2% |
| D | 0,3 | 5,3 | 165 | 0% | 3% |
Thus, it is worthwhile to search for compression of the mesenteric and splenic veins in cachectic patients (BMI <20) with severe, postprandial abdominal pain localized in the right upper quadrant, diarrhea, and the need for parenteral nutrition due to an inability to be sufficiently nourished by the oral route.
Treatment:
Patient D underwent successful surgery and experienced post-operative relief from post-prandial pain. Her pancreatic collaterals disappeared within four weeks after the operation. Intraoperatively, a superior mesenteric vein embedded in thick layers of connective tissue was found. Removing the connective tissue resulted in decompression of the superior mesenteric vein and complete normalisation of the venous flow pattern in colour Doppler sonography..
Discussion
Habitual compression syndromes of the mesenteric and splenic veins at their confluence to form the portal vein have not been described in the literature thus far. A pubmed search with the search words: superior mesenteric vein compression in title revealed 2 papers:[1, 2]
Mesenteric vein compression is comparable to stenosis in terms of its hemodynamic and functional intestinal consequences. A report of three cases of superior mesenteric vein (SMV) stenosis due to inflammatory damage in Crohn’s disease revealed that the presenting symptoms were gastrointestinal bleeding in two cases and pain and diarrhea in the third case. In one case of idiopathic SMV stenosis, the patient presented with melena and hematemesis. Another case report describes postoperative SMV stenosis causing intestinal edema [5]. SMV stenosis occurs more frequently in liver transplantation. In another series of six patients, the stenosis was caused by pancreatitis, postoperative strictures, and pancreatic carcinoma. The presenting symptoms were symptomatic ascites, mesenteric ischemia, and recurrent gastrointestinal bleeding. Bleeding from duodenal varices, which developed due to superior mesenteric vein stenosis as a consequence of recurrent pancreatitis, was treated with intravenous stenting. Stenting from different access points is the most frequently applied treatment (5, 8–13).
The cases described in the literature required acute intervention due to life-threatening complications from high-grade inflammatory, malignant, stenotic, or thrombotic superior mesenteric vein conditions.
Our cases are quite different. Our patients have suffered for many years from slowly increasing abdominal pain and weight loss, in the absence of acute mesenteric vein obstruction. In two of our patients (C and D), collateral circulation encompassing the pancreas could be demonstrated.
The dominant features were massive weight loss, pain, disturbed bowel motility, an inability to eat, and bloating as a sign of disturbed nutrient absorption.
These symptoms are nonspecific, so compression of the superior mesenteric vein is rarely considered.
However, a detailed color Doppler sonography can detect the condition and describe the functional impact of varying degrees of superior mesenteric venous outflow obstruction. The pressure gradient provides an indication of the severity of the obstruction, but the new 4D-PixelFlux volume flow measurement of the superior mesenteric vein’s transport capacity before and after a meal is a promising tool for gauging the obstruction’s impact on small bowel function. When searching for unusual venous compressions, it is highly advisable to use color scales that depict turbulences. While conventional color Doppler ultrasound only depicts flow direction and velocity in various shades of red or blue, the variance mode adds green and yellow to highlight turbulences, which are a sign of disturbed flow patterns and a hallmark of vessel narrowing. Thus, with a large color window, even small vascular anomalies stand out.
Conclusion
For patients experiencing chronic, unexplained weight loss; postprandial abdominal pain; and signs of impaired small bowel motility or absorption, habitual compression of the superior mesenteric vein should be considered. Surgical correction is feasible.
Literature
- Genser, L., P.A. Colas, and C. Barrat, Superior mesenteric vein compression: A reliable sign of internal hernia after gastric bypass. Surg Obes Relat Dis, 2019. 15(4): p. 666–667.
- Maier, J., A. Herrasti Gallego, and A.K. Floyd, Compression of the superior mesenteric vein-a sign of acute internal herniation in patients with antecolic laparoscopic Roux-en-Y gastric bypass. Eur Radiol, 2017. 27(4): p. 1733–1739.
- Hodgson, R.S., et al., Superior mesenteric vein stenosis complicating Crohn’s disease. Gut, 1999. 45(3): p. 459–62.
- Grasu, M.C., et al., Endovascular Stenting for Idiopathic Stenosis of the Superior Mesenteric Vein: A Case Report. Diagnostics (Basel), 2024. 14(11).
- Lin, C., et al., Percutaneous transhepatic stenting for acute superior mesenteric vein stenosis after pancreaticoduodenectomy with portal vein reconstruction: A case report. World J Gastrointest Surg, 2024. 16(4): p. 1195–1202.
- Beyer, L.P., et al., Percutaneous treatment of symptomatic superior mesenteric vein stenosis using self-expanding nitinol stents. Eur J Radiol, 2015. 84(10): p. 1964–9.
- Bhat, A.P., R.M. Davis, and W.D. Bryan, A rare case of bleeding duodenal varices from superior mesenteric vein obstruction -treated with transhepatic recanalization and stent placement. Indian J Radiol Imaging, 2019. 29(3): p. 313–317.
- Hellman, P., et al., Stenting of the superior mesenteric vein in midgut carcinoid disease with large mesenteric masses. World J Surg, 2010. 34(6): p. 1373–9.
- Kelay, A., et al., Retrograde Stenting Under Transmesenteric Angiographic Guidance of an Occluded Superior Mesenteric Vein to Treat Life-Threatening Hemorrhage. Ann Vasc Surg, 2016. 31: p. 209 e11–5.
- Sun, X., L. Wang, and H. Qian, Relief of symptoms after stent placement for superior mesenteric vein stenosis following abdominal radiation therapy. Asian J Surg, 2023.
- Kirk, T., et al., Superior Mesenteric Vein Stenting to Manage Persistent Chylothorax. Cardiovasc Intervent Radiol, 2024. 47(9): p. 1299–1302.
- Cao, G., et al., Treatment of postoperative main portal vein and superior mesenteric vein thrombosis with balloon angioplasty and/or stent placement. Acta Radiol, 2013. 54(5): p. 526–32.
- Argiro, R., et al., Percutaneous transhepatic stent for chronic intestinal bleeding from jejunal varices in primary idiophatic superior mesenteric vein stenosis: A case report. Radiol Case Rep, 2022. 17(4): p. 1271–1275.