- New stuff to read and discuss
- What patients say
- Clinic / online appointments
- Why the diagnosis of a psychosomatic illness is often a misdiagnosis
- Vascular Compression Syndromes
- Do you have questions?
- Checklist vascular compression syndromes
- Description of your symptoms
- Researchers from the Mayo Clinic confirm my concept of the Midline Congestion Syndrome
- Explanation of gender-specific differences in the clinical symptoms of abdominal vascular compression syndromes: varicocele and penile/testicular pain – their main manifestation in men.
- Varicocoele is predominantly caused by left renal vein compression
- Musculoskeletal pecularities of female puberty
- Lordosis /Swayback- Origin of many abdominal compression syndromes
- Bending of a straight vein compels its narrowing
- The lordogenetic midline congestion syndrome
- Neurological consequences of the midline congestion syndrome
- Successful treatment of a teenage girl who was unable to eat due to extreme postprandial pain and unable to walk due to spasticity in her left leg
- Severe ataxia in a young woman with severe spinal congestion – complete resolution after decompression of the left renal vein
- All compression syndromes are one: the spectrum of lordogenetic compressions
- Nutcracker-Syndrome is a misnomer! Lordogenetic left renal vein compression is a more appropriate name!
- May-Thurner-constellation (May-Thurner-syndrome, Cockett’s syndrome)
- Midline (congestion) syndrome
- Pelvic congestion syndrome
- Celiac Trunk Compression / Dunbar syndrome / MALS / Arcuate ligament syndrome
- Wilkie-Syndrome / Superior-mesenteric-artery-syndrome
- Compression of the vena cava inferior
- Evlauation of vascular compressions with the PixelFlux-method
- Connective tissue disorders predispose to multiple compressions
- Postural tachycardia syndrome (POTS) – the hemodynamic consequence of vascular compression syndromes and loose connective tissue
- Restless legs-a little known symptom of abdominal vascular compression syndromes
- Pudendal neuralgia in vascular compression syndromes
- A new sonographic sign of severe orthostatic venous pooling
- Migraine and Multiple Sclerosis
- Hemodynamic effect on cerebral perfusion in patients with multiple localised vascular compression.
- Treatment of vascular compression syndromes
- Fatal errors in the treatment of vascular compression syndromes
- Risks of stents in venous compression syndromes
- Surgical treatment of abdominal compression syndromes: The significance of hypermobility‐related disorders
- Nutcracker and May-Thurner syndrome: Decompression by extra venous tube grafting and significance of hypermobility related disorders
- Our surgical treatment of vascular compressions
- Chronic regional pain syndrome (CRPS) caused by venous compression and mechanical irritation of the coeliac plexus
- Vascular compression syndromes and other disease mechanisms I recently detected
- Kaleidoscope of instructive cases
- Venous congestion of the spinal cord may be a potential contributor to the development of paraplegia in patients with spinal muscular atrophy type III (Kugelberg-Welander disease)
- Ultrasound Diagnostics
- A breakthrough in functional sonographic diagnostic – 4D-colour Doppler sonographic flow volume measurements
- 4D-volume flow measurements of jugular and mesenteric veins
- Inauguration of the global volumetric brain perfusion measurement-a gateway for understanding of neurological symptoms
- Ultrasound focused entirely on all of your symptoms
- Ultrasound vs. X-ray
- Vascular Malformations
- Profile
- Functional colour Doppler ultrasound – how I do it
- Perfusion Measurement – PixelFlux-method
- Research
- Publications
- Nutcracker and May-Thurner syndrome: Decompression by extra venous tube grafting and significance of hypermobility related disorders
- Papers authored by Th. Scholbach
- Publications
- Inauguration of measurements of the tissue pulsatility index in renal transplants
- From nutcracker phenomenon to midline congestion syndrome and its treatment with aspirin
- First sonographic tissue perfusion measurement in renal transplants
- First sonographic bowel wall perfusion measurement in Crohn disease
- First sonographic renal tissue perfuison measurement
- First sonographic measurement of renal perfusion loss in diabetes mellitus
- PixelFlux measurements of renal tissue perfusion
- Why I prefer not to publish in journals but in the Internet
- Vessel stretching in nephroptosis – an important driver of complaints
- Publications
- Expertise
- Bornavirus Infection
- Scientific cooperation
- Cookie Policy
- Data protection
- Cookie Policy (EU)
- Impressum
A new type of duodenal obstruction as a consequence of its compression by the post-prandially enlarging stomach
I am going to describe here, the best of my knowledge, for the first time a unique case where the enlarging stomach after a meal was compressing the duodenum thus obstructing the transport of food across the horizontal portion of the duodenum with subsequent epigastric pain, sensation of disturbed transport of food and a rapidly increasing congestion of the lower body due to a compression of the vena cava inferior by the enlarging duodenum.
The patient suffered from epigastric pain after ingestion of food or even fluid at the level of 5-7/10 every day. She describes nausea and a feeling as if the food is stuck in the upper abdomen. She also has pain in the left groin and increasingly in the left flank, swelling in the left leg, bladder problems, frequent urinary tract infections (bacteriuria, proteinuria, leukocyturia – after antibiotic treatment short but not lasting improvement, dysuria after prolonged sitting or walking in the evening), pain in the lower back, dizziness and vertigo on standing up, poor concentration, headaches, tired easily, sweating, pain in the upper abdomen, skipped heartbeats, extreme postprandial palpitations and sweating, also on standing – always extreme dizziness.
In the patient’s words: “After eating, or even during (it varies depending on what I eat), I have a severe cramp-like, pressing pain in the middle where the ribs begin to separate. Sometimes it is a little further below the described location. But there it feels more like someone is pressing their fist really hard on my stomach and then pulling under my left rib, causing a ripping sensation. Up to the left flank. And then it can sometimes be felt between the shoulder blades. I start to sweat and feel tightness in the left chest area and my heart starts to race and double-beat. Dizziness sets in and I could fall asleep on the spot. I often have the feeling that the food is still stuck in my esophagus. I sometimes notice, when I drink something later, about 15 or 20 minutes later, that something still slides down while drinking. I can’t describe it any differently. It often gives me a feeling of being compressed in the chest when drinking. Heavy, tight, pressure. These are the terms that come to mind. I have gained weight because I force myself to eat. I usually have no appetite. However, I have developed a real disgust for some foods. But I also get pain in the upper abdomen independently of eating. And then when I sit for a longer period of time, the pain is more of a constant pressure pain, in the middle it sometimes starts to throb strongly.”
On presentation there is spontaneous pain in the left mid-abdomen and left flank, and on palpation of the abdomen there is additional pain in the left renal region and at the left inguinal ligament. No pathological resistance is palpable. The joints are partially hyperextensible, especially the elbows. The Beighton score is 5/9. Striae distensae are not visible. Genetic diagnosis reveals clinically hypermobile Ehlers-Danlos syndrome. Auscultation reveals no vascular murmurs and normal peristalsis.
After ingestion, there is immediate and massive gas formation in the duodenum and stomach. As a result, the protruding greater curvature of the stomach compresses the horizontal duodenal segment against the aorta. The superior mesenteric artery lies 15 mm from the aorta on the right paramedian and cannot contribute to the compression of the duodenum. However, the compression of the horizontal portion of the duodenum by the stomach impedes the transport of food in the duodenum, causing the distended duodenum to press against the vena cava and reduce its cross-sectional area from 1.35 cm² before the uptake of food to 0.29 cm² after a meal. This obstructs recirculation from the pelvis, as evidenced by a reduction in perfusion of the left internal iliac vein from 265 mL/min before the meal to 116 ml/min after the meal .
At the same time, as described above, blood flow to the left kidney decreases significantly, especially in the standing position due to the simultaneous compression of the left renal vein by the stomach.
Within the sonographic examination, the discomfort could be explained by a unique mechanism:

The gap between stomach and the aorta is wide as long as the stomach is empty. In such a situation the reason for the patient’s symptoms would not be visible.

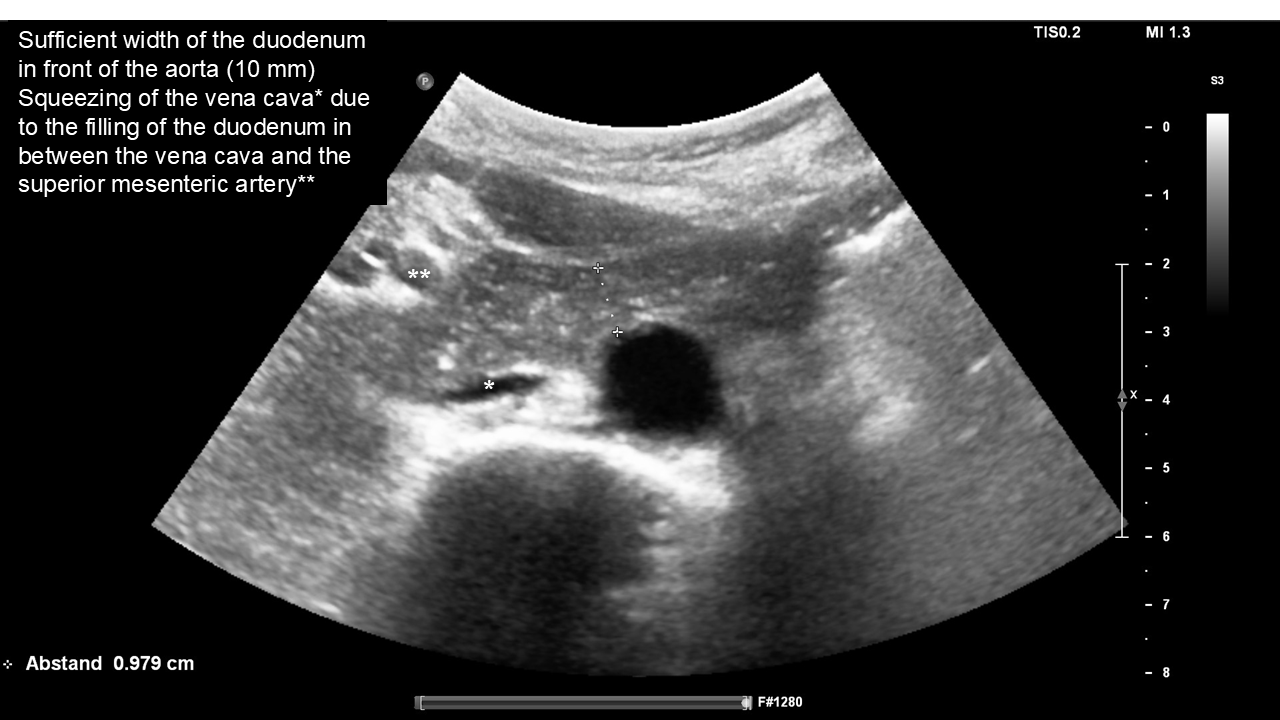
The duodenum is not compressed in front of the aorta nor between the aorta and the superior mesenteric artery which lies far to the right of the aorta. However, the beginning filling of the duodenum is already squeezing the vena cava.
The duodenum is compressed by the expanding stomach against the left circumference of the aorta. The stomach had become distended due to a sudden production of gas in the duodenum and stomach immediately after the mucosa came into contact with the ingested food. The compression of the duodenum caused distension of its more oral part.

This distension in turn compresses the vena cava, thereby significantly reducing the venous return to the heart after a meal. This was the cause of a vena cava syndrome with the typical symptoms: Tachycardia, lower abdominal pain, a feeling of fainting and dizziness, and severe upper abdominal pain. The pain radiated to the left groin, specifically due to the additional compression of the left renal vein by the expanding stomach.

It is not uncommon for the left renal vein and duodenum to be compressed simultaneously as they both pass between the superior mesenteric artery and the aorta. A common combination is superior mesenteric artery syndrome (Wilkie syndrome) with compression of the left renal vein (lordogenetic left renal vein compression, also known as nutcracker syndrome).
The compression of the left renal vein forces additional volume to flow down the left ovarian vein, which enters the pelvic circulation on the left side. This is the reason why the patient experienced a specific pain localisation in the left groin area, due to the double effect of the additional pressurisation of both iliac veins due to the postprandial compression of the vena cava on the one hand, and the volume overload specifically of the left pelvic area due to the collateralisation of the additional blood volume from the left renal vein on the other hand.
This can be clearly demonstrated by PixelFlux measurements of the renal perfusion which demonstrates a significant reduction of the left renal perfusion while standing after a meal by 55%!

PixelFlux measurement of the renal parenchymal perfusion in 3 layers of the kidney showing a reduction of the left renal perfusion after a meal by 55% due to the compression of the left renal vein by the enlarging stomach simultaneously with the above-described compression of the duodenum due to the same mechanism.