- New stuff to read and discuss
- What patients say
- Clinic / online appointments
- Why the diagnosis of a psychosomatic illness is often a misdiagnosis
- Vascular Compression Syndromes
- Do you have questions?
- Checklist vascular compression syndromes
- Description of your symptoms
- Researchers from the Mayo Clinic confirm my concept of the Midline Congestion Syndrome
- Explanation of gender-specific differences in the clinical symptoms of abdominal vascular compression syndromes: varicocele and penile/testicular pain – their main manifestation in men.
- Varicocoele is predominantly caused by left renal vein compression
- Musculoskeletal pecularities of female puberty
- Lordosis /Swayback- Origin of many abdominal compression syndromes
- Bending of a straight vein compels its narrowing
- The lordogenetic midline congestion syndrome
- Neurological consequences of the midline congestion syndrome
- Successful treatment of a teenage girl who was unable to eat due to extreme postprandial pain and unable to walk due to spasticity in her left leg
- Severe ataxia in a young woman with severe spinal congestion – complete resolution after decompression of the left renal vein
- All compression syndromes are one: the spectrum of lordogenetic compressions
- Nutcracker-Syndrome is a misnomer! Lordogenetic left renal vein compression is a more appropriate name!
- May-Thurner-constellation (May-Thurner-syndrome, Cockett’s syndrome)
- Midline (congestion) syndrome
- Pelvic congestion syndrome
- Celiac Trunk Compression / Dunbar syndrome / MALS / Arcuate ligament syndrome
- Wilkie-Syndrome / Superior-mesenteric-artery-syndrome
- Compression of the vena cava inferior
- Evlauation of vascular compressions with the PixelFlux-method
- Connective tissue disorders predispose to multiple compressions
- Postural tachycardia syndrome (POTS) – the hemodynamic consequence of vascular compression syndromes and loose connective tissue
- Restless legs-a little known symptom of abdominal vascular compression syndromes
- Pudendal neuralgia in vascular compression syndromes
- A new sonographic sign of severe orthostatic venous pooling
- Migraine and Multiple Sclerosis
- Hemodynamic effect on cerebral perfusion in patients with multiple localised vascular compression.
- Treatment of vascular compression syndromes
- Fatal errors in the treatment of vascular compression syndromes
- Risks of stents in venous compression syndromes
- Surgical treatment of abdominal compression syndromes: The significance of hypermobility‐related disorders
- Nutcracker and May-Thurner syndrome: Decompression by extra venous tube grafting and significance of hypermobility related disorders
- Our surgical treatment of vascular compressions
- Chronic regional pain syndrome (CRPS) caused by venous compression and mechanical irritation of the coeliac plexus
- Vascular compression syndromes and other disease mechanisms I recently detected
- Kaleidoscope of instructive cases
- Venous congestion of the spinal cord may be a potential contributor to the development of paraplegia in patients with spinal muscular atrophy type III (Kugelberg-Welander disease)
- Ultrasound Diagnostics
- A breakthrough in functional sonographic diagnostic – 4D-colour Doppler sonographic flow volume measurements
- 4D-volume flow measurements of jugular and mesenteric veins
- Inauguration of the global volumetric brain perfusion measurement-a gateway for understanding of neurological symptoms
- Ultrasound focused entirely on all of your symptoms
- Ultrasound vs. X-ray
- Vascular Malformations
- Profile
- Functional colour Doppler ultrasound – how I do it
- Perfusion Measurement – PixelFlux-method
- Research
- Publications
- Nutcracker and May-Thurner syndrome: Decompression by extra venous tube grafting and significance of hypermobility related disorders
- Papers authored by Th. Scholbach
- Publications
- Inauguration of measurements of the tissue pulsatility index in renal transplants
- From nutcracker phenomenon to midline congestion syndrome and its treatment with aspirin
- First sonographic tissue perfusion measurement in renal transplants
- First sonographic bowel wall perfusion measurement in Crohn disease
- First sonographic renal tissue perfuison measurement
- First sonographic measurement of renal perfusion loss in diabetes mellitus
- PixelFlux measurements of renal tissue perfusion
- Why I prefer not to publish in journals but in the Internet
- Vessel stretching in nephroptosis – an important driver of complaints
- Publications
- Expertise
- Bornavirus Infection
- Scientific cooperation
- Cookie Policy
- Data protection
- Cookie Policy (EU)
- Impressum
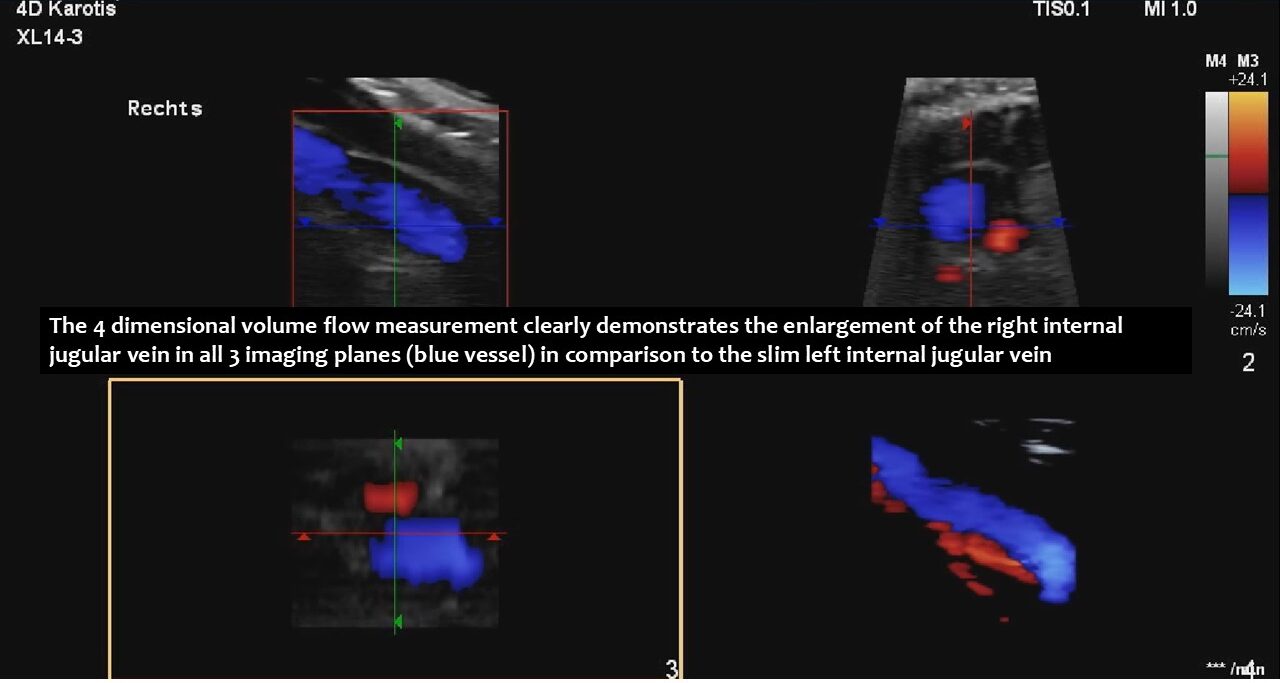
4-D volume flow measurements of the jugular veins reveal the origin of extreme positional headaches
4-D volume flow measurements of the jugular veins reveal the origin of extreme positional headaches in a patient with abdominal, pelvic and cervical venous compression syndromes
This is a 36-year-old female patient with hypermobile Ehlers-Danlos syndrome (hEDS) and extreme positional headaches, which can be explained by functional, qualitative and four-dimensional ultrasound. The headaches are a consequence of the pressurisation of the skull.
The increased intracranial pressure caused debilitating headaches and disturbed vision.
These headaches changed with body and head posture.
The cause was compression of the left renal vein, the left common iliac vein, both jugular veins and the left cephalic vein.
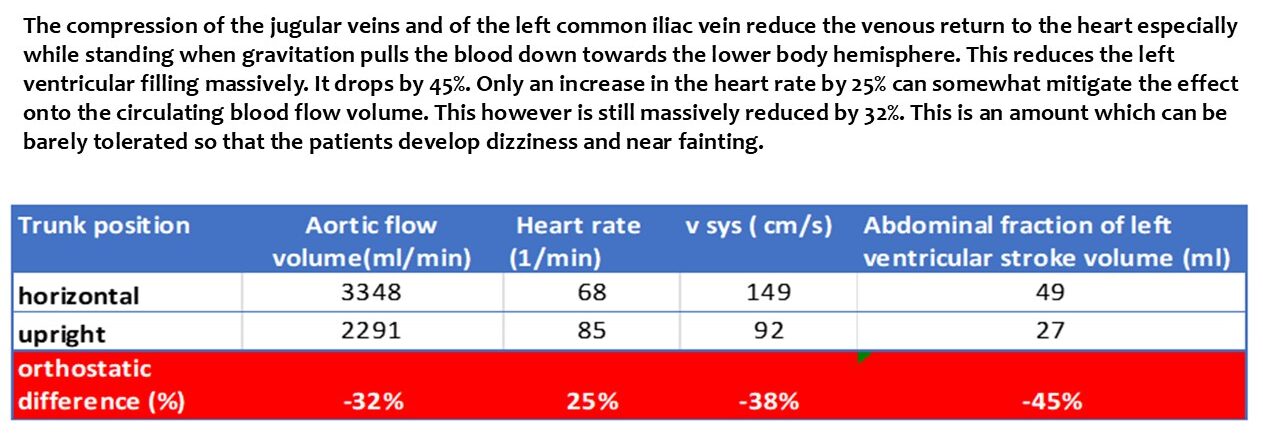
The main driving force was the compression of the left renal vein, as this vein transports most of the blood in the lower body hemisphere. Compression of this vein forces blood to run down the left ovarian vein towards the left internal and common iliac veins. The blood then tries to cross the spine to reach the inferior vena cava. This vessel returns blood to the heart. However, in this patient, the left common iliac vein was also compressed. Consequently, the increased pressure in the left renal vein could only be relieved by creating an additional collateral pathway. This connects the left renal vein with the spinal canal and is called tronc réno-rachidièn .
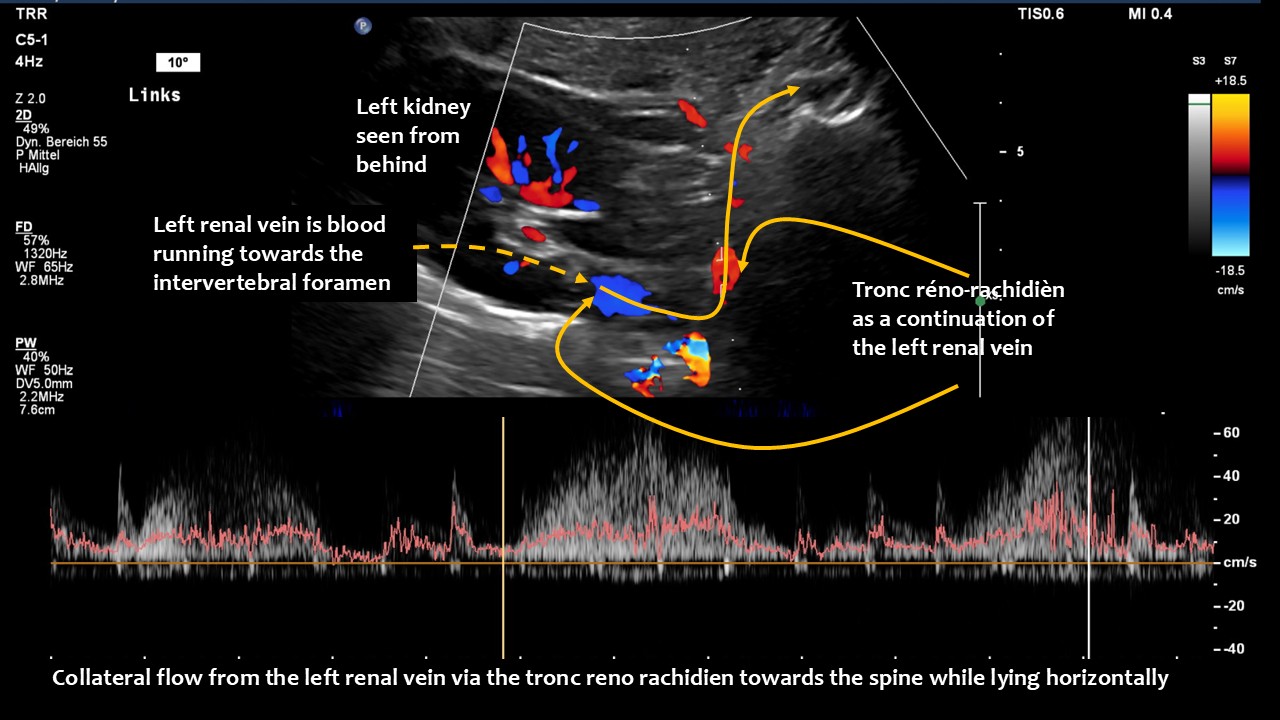

Large volumes of blood from the left renal vein enter the spinal canal and run along the spinal veins (epidural plexus) towards the skull, entering the intracranial sinuses. They can then leave the skull via the vertebral veins, but mainly via the jugular veins.
The vertebral veins are not helpful in this process, as they run inside bony rings along the cervical vertebrae. These bony rings prevent these veins from enlarging, which would be necessary to take up the additional blood from the skull.
Therefore, the jugular veins are the main escape route for the additional blood from the skull that stems from the left renal vein.
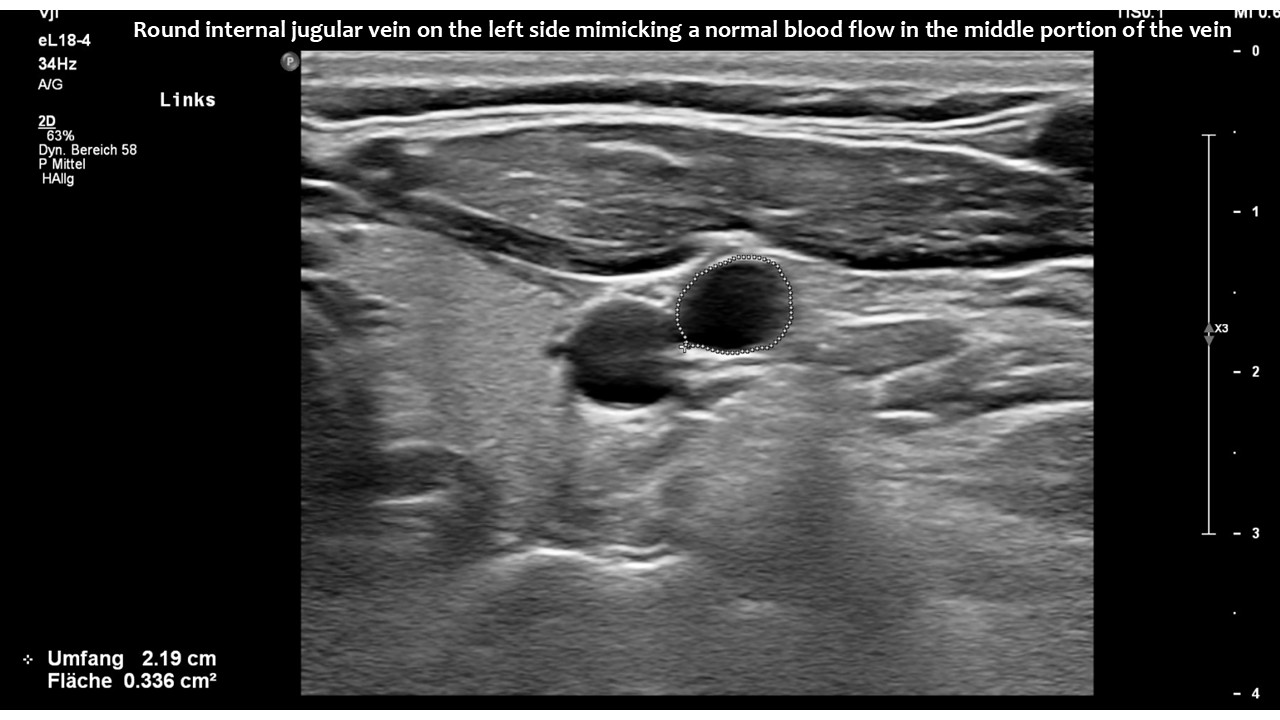
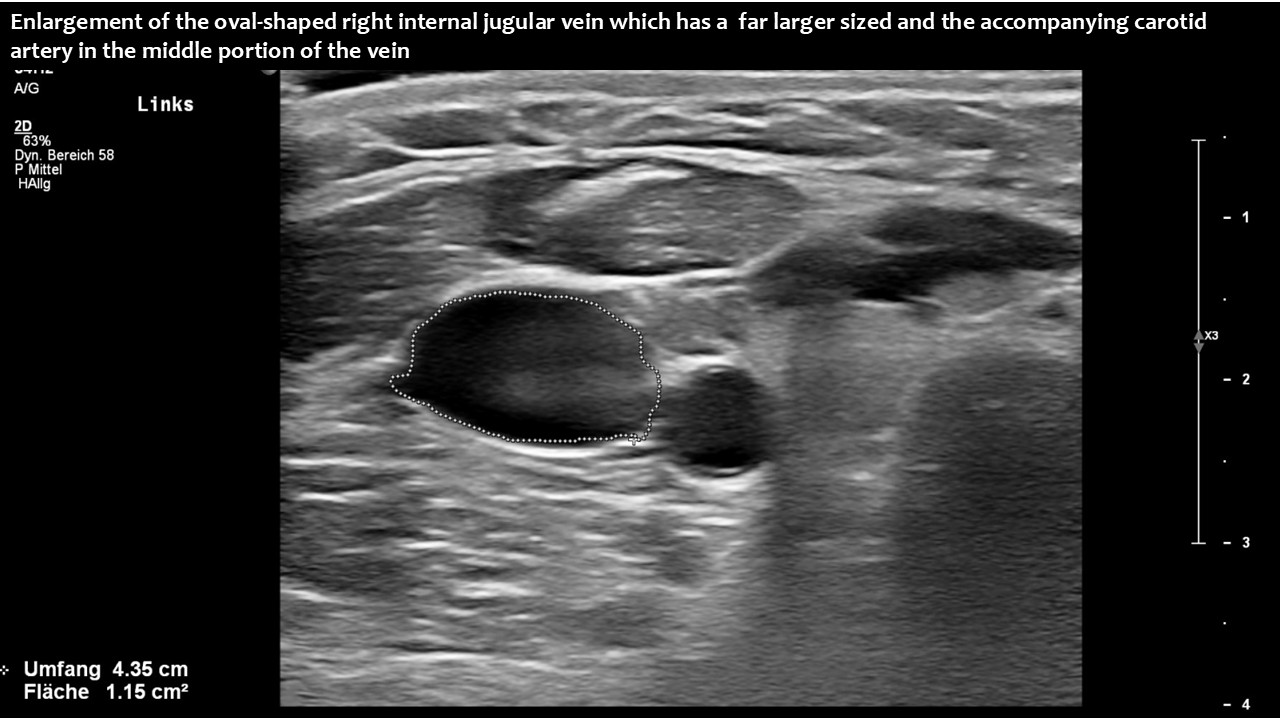
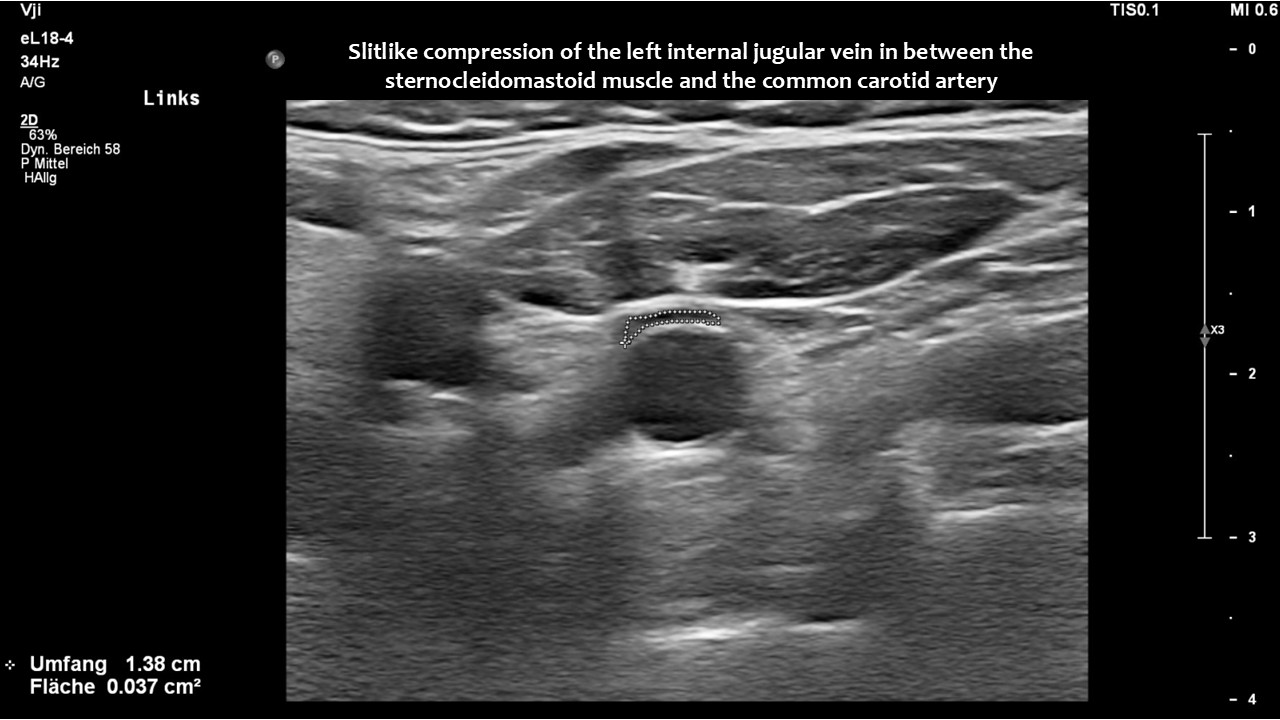
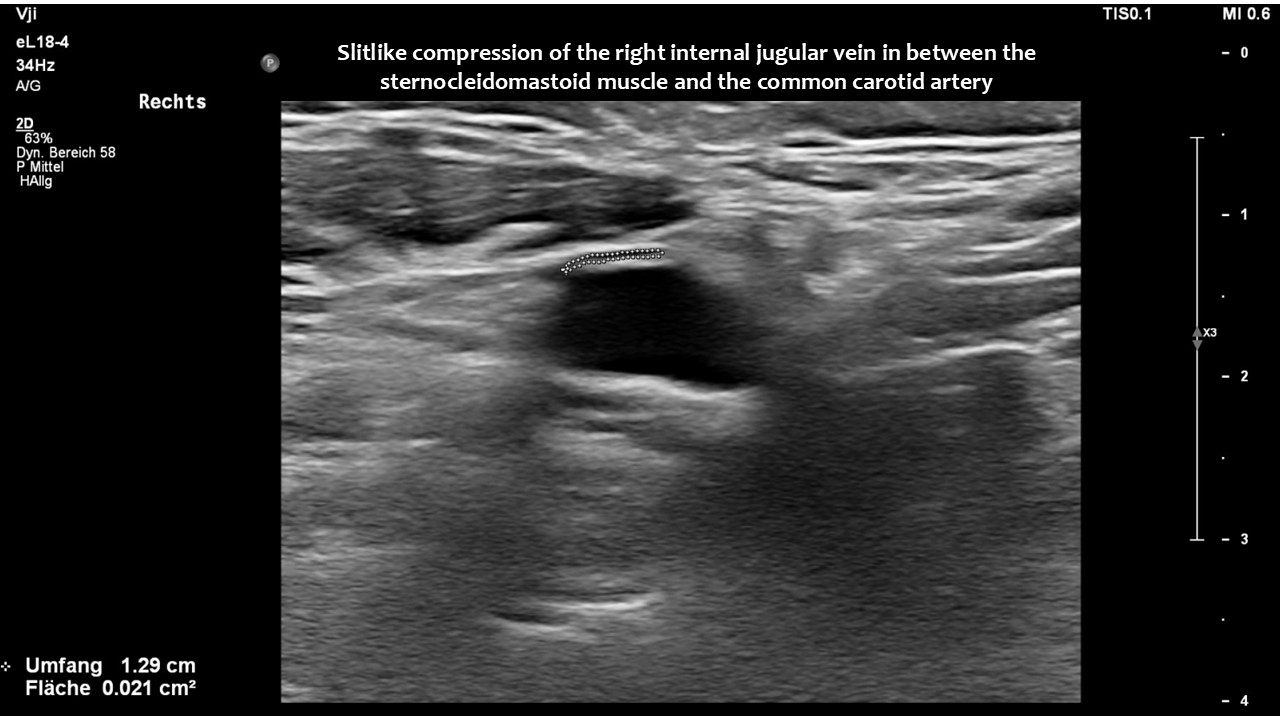
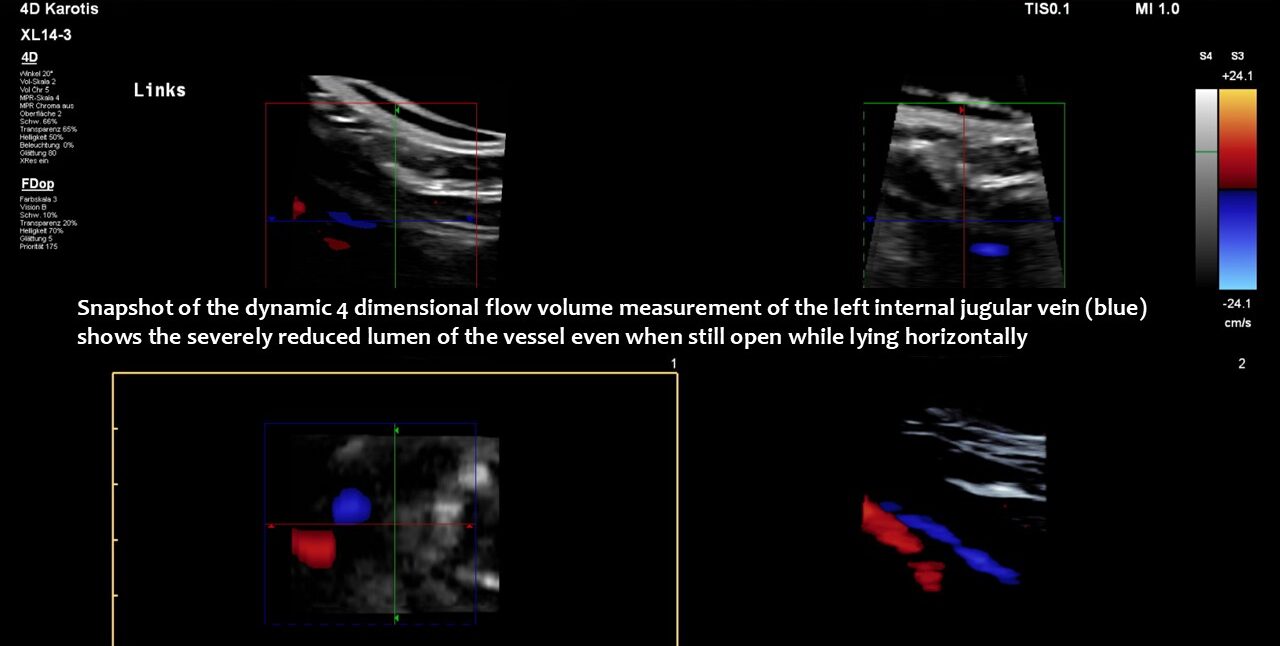
However, in this patient, both jugular veins were compressed. The middle portion of the internal jugular vein was pushed ventrally by the increased cervical lordosis on both sides, becoming squeezed between the carotid artery and the sternocleidomastoid muscle.
Increased cervical lordosis is a very common feature in patients with EDS. This increased curvature is necessary for compensating for the increased lumbar lordosis and thoracic kyphosis in these patients.
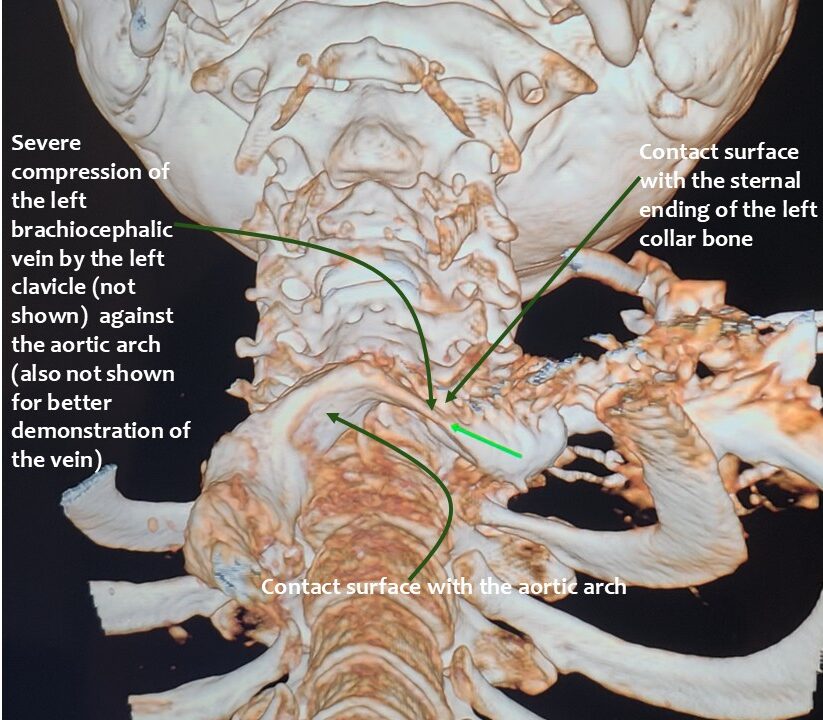
In addition, the patient had compression of the left brachiocephalic vein.
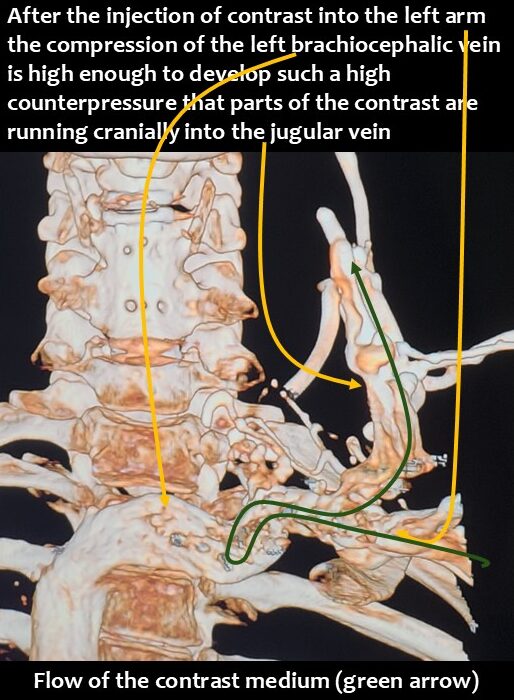
Consequently, blood had difficulty leaving the skull, resulting in continuously increased pressure and severe headaches, as well as other neurological dysfunction. The left side was more affected due to the double compression. This was clearly demonstrated by four-dimensional volume flow measurements in both jugular veins.
 Only a four-dimensional volume flow measurement of the jugular veins can determine the cause of the daily headaches. The overall reduction in venous outflow from the brain in both jugular veins, totalling 258 mL/min, is significantly lower than the normal average volume of 719 mL/min. Consequently, the patient can eliminate only 36% of the required flow volume, while additional volume is forced into the skull from the left renal vein via the tronc réno-rachidien and from the left common iliac vein via the left ascending lumbar vein. This results in a chronic increase in intracranial pressure, as demonstrated by the elevated cerebrospinal fluid pressure obtained through a lumbar puncture. When the left jugular vein is also completely compressed due to increasing cervical lordosis when upright, the headaches become unbearable, accompanied by additional neurological symptoms as described by the patient.
Only a four-dimensional volume flow measurement of the jugular veins can determine the cause of the daily headaches. The overall reduction in venous outflow from the brain in both jugular veins, totalling 258 mL/min, is significantly lower than the normal average volume of 719 mL/min. Consequently, the patient can eliminate only 36% of the required flow volume, while additional volume is forced into the skull from the left renal vein via the tronc réno-rachidien and from the left common iliac vein via the left ascending lumbar vein. This results in a chronic increase in intracranial pressure, as demonstrated by the elevated cerebrospinal fluid pressure obtained through a lumbar puncture. When the left jugular vein is also completely compressed due to increasing cervical lordosis when upright, the headaches become unbearable, accompanied by additional neurological symptoms as described by the patient.
Without this sophisticated technique, it would be unclear how severe the pressurization of the skull was and that, despite compression of both jugular veins, the right one was the main escape route from the skull.
Measuring transcranial flow velocity in the intracranial arteries could provide evidence of localised brain pressurisation effects by demonstrating increased vascular resistance in the left posterior cerebral artery while sitting. This artery supplies the visual cortex. The patient suffered from severe visual disturbances.
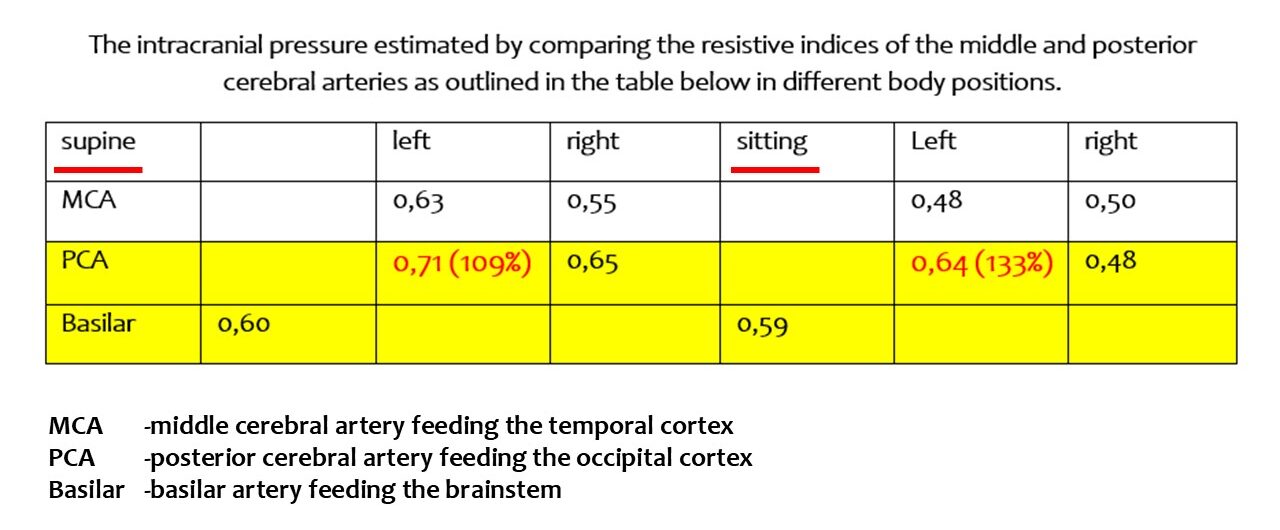
This occurred when the patient experienced more severe headaches. This was because the outflow from the left jugular vein was completely blocked as soon as the patient sat up, affecting the left posterior cerebral artery. This could only be demonstrated using 4D volume flow measurements of both jugular veins in different patient positions.