Leg pain is very common, starting in early childhood. Rarely, disturbed blood flow is considered in pain and tension if swelling of the leg is absent.
I will therefore report four cases: one of a 38-year-old woman with a bluish swelling in her left leg when standing, which disappeared when lying down and a 39-year-old lady with bilateral leg pain and paraparesis and of a six-year-old girl who was unable to stand for long due to increasing pain and tension in the lower legs, and chronic bilateral leg pain mainly in the back of the knees and a 12 year old girl with week and aching legs.
Adult patients
A 38-year-old female patient with a history of bilateral hip dysplasia, who was treated with pelvic osteotomy and subsequently developed thrombosis in her right leg, presented with posture-dependent bluish swelling of her left leg and foot. This was accompanied by hyperalgesia, pins and needles, and postural tachycardia.
Clinical examination revealed no abnormalities except for hypermobility with a Beighton score of 5/9, and both legs were painful at a level of 3/10, 24 hours a day.
Functional colour Doppler sonography revealed severe orthostatic venous pooling, reducing left ventricular filling by 56% when standing. This was accompanied by an increase in heart rate from 100 to 160 bpm when changing from a horizontal to an upright posture, but this did not prevent a 30% drop in aortic flow volume. This explains the patient’s postural tachycardia.
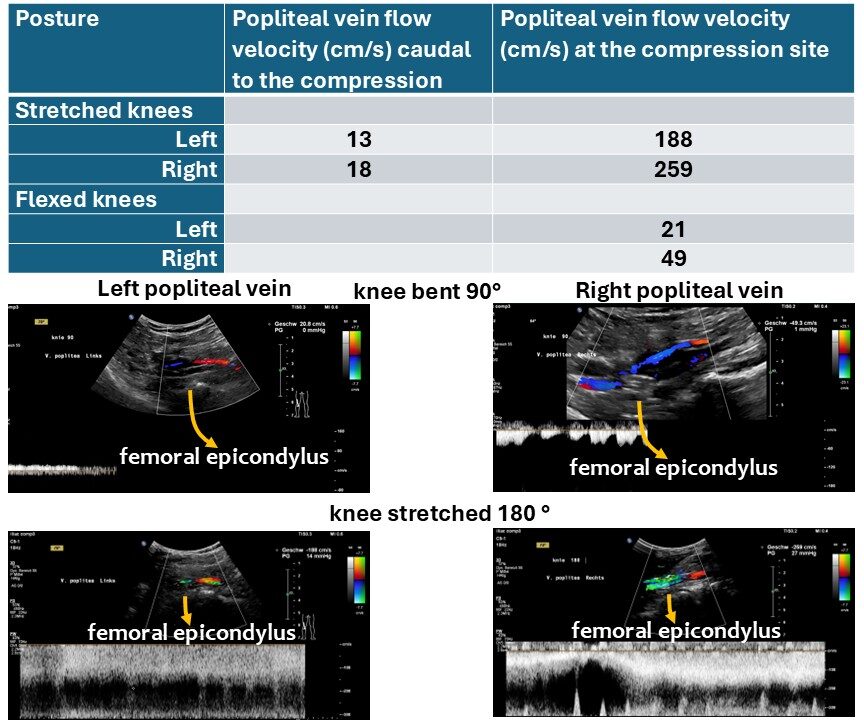
Due to the noticeable discolouration of the calves, the popliteal vein was also examined. With the knees extended, severe compression of the popliteal vein was observed on both sides, albeit at different locations. On the left, compression occurred immediately dorsal to the tibial plateau; on the right, it occurred dorsal to the femoral epicondyles.
On the right, the vein shifts dorsally when a muscle belly interposes itself between the femoral condyles and the vein, resulting in decompression of the vein. On the left, the compression disappears upon flexion, as this counteracts the stretching of the vein across the tibial plateau.
A 39-year-old female patient presented with constant pain in both legs rated at 10/10, and an inability to walk due to weakness in both legs, which was slightly more severe on the right side. She also exhibited clear signs of hypermobility disorder, with a Beighton score of 8/9, and arrived by wheelchair.
She could not spontaneously move her right leg. Home neurological diagnostics, including a functional neurological examination with EMG and evoked potentials, as well as an MRI scan of the brain and spine, did not reveal any cause for this painful paralysis of the legs.
Functional sonographic diagnostics revealed May–Thurner syndrome, resulting in congestion in both legs. This was due to simultaneous outflow obstruction from the left pelvic hemisphere and flooding of the right pelvic hemisphere, hindering upstream flow from the right external iliac vein.
Furthermore, significant compression of the left renal vein was observed, accompanied by spinal congestion, as evidenced by pulsatile lumbar venous outflow from the spine at the level of the 11th rib. This was interpreted as resulting from intraspinal influx due to the congested and rhythmically compressed left common iliac vein, caused by compression from the crossing right common iliac artery transferring the arterial pulse into the spinal collateral circulation. This massive spinal congestion was likely the cause of the bilateral leg paralysis.
Pediatric patients
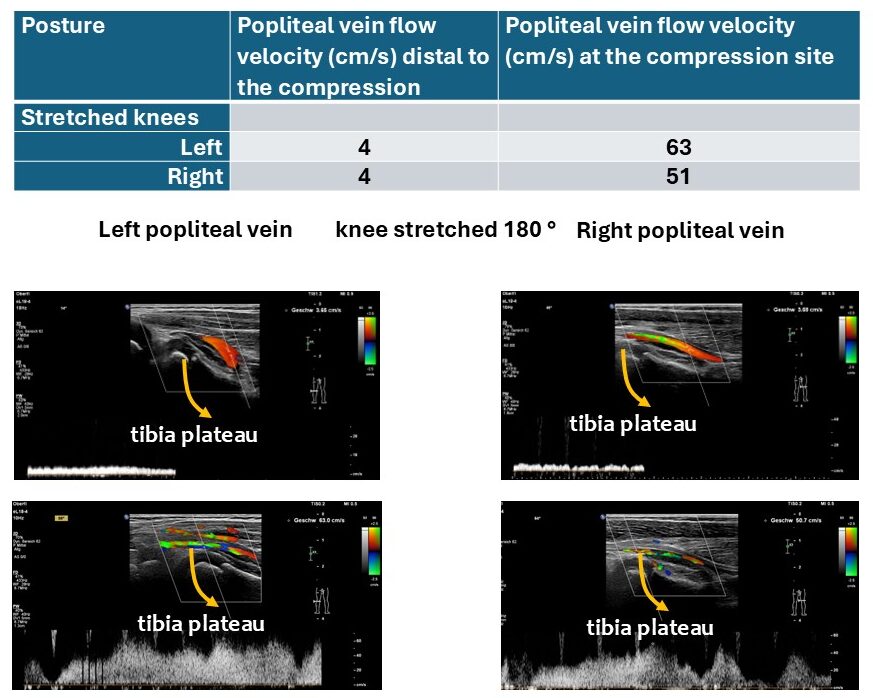
In a six-year-old girl, both knee joints were unremarkable, with no effusion and normal cartilage. However, the popliteal veins were severely compressed when the knees were stretched, due to hypermobile joints as part of a hypermobility disorder, likely hypermobile Ehlers-Danlos syndrome (hEDS). Flow acceleration was observed in the left popliteal vein due to compression, increasing from 4.1 cm/s below the knee to 51 cm/s behind the tibial plateau. At the same level, the respective measurements on the right knee were 3.7 cm/s and 63 cm/s. This clearly indicates an obstruction to venous outflow from the calves when the child’s knees are stretched. This explains why the child cannot stand or walk for long due to venous congestion in the calves, which causes pain and tension.
Another girl, aged 12, with hypermobile joints and a Beighton score of 6/9, mainly suffered from weakness and an aching pain in both legs, which was sometimes more prominent on the right side than the left and increased while standing. Her legs did not swell, and she also had POTS symptoms. She faints after standing upright for 15 minutes, feels weak after standing for a while, and takes several days to recover.
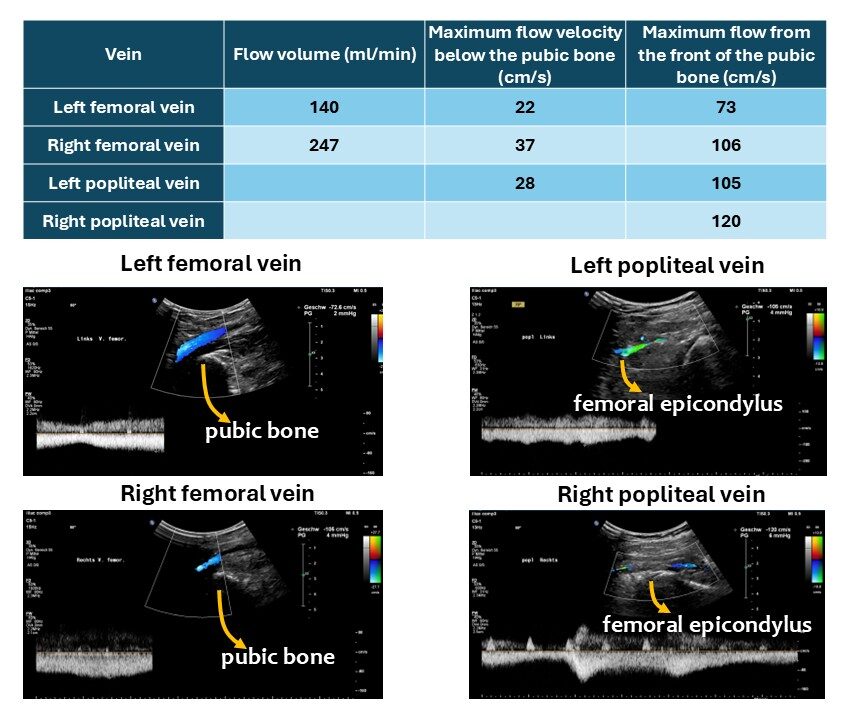
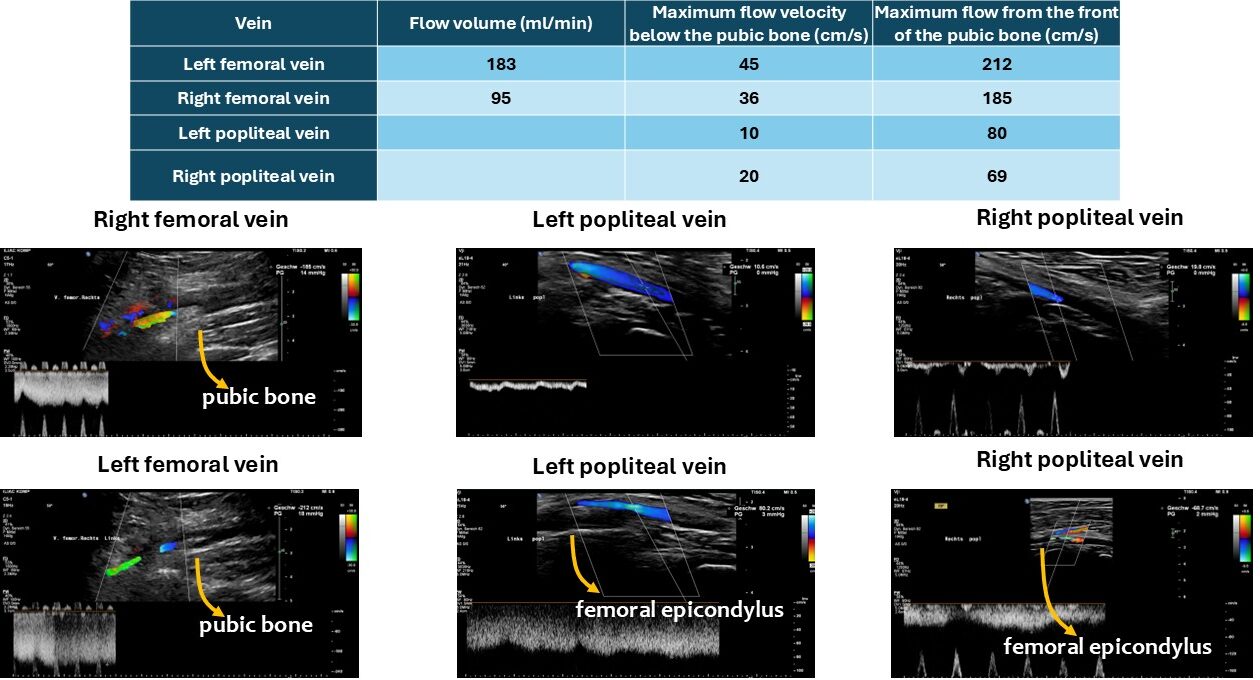
While standing she developed a reduction of the left ventricular filling by 56% but an only moderate increase of the heart rate from 65-81/min which could not compensate for the massive orthostatic venous pooling and thus resulting into a reduction of the circulating aortic flow volume by 45%. This explains the postural tachycardia with inability to stand for more than 15 minutes and constant brain fog episodes of near fainting. Beside a compression of the popliteal veins also the femoral veins were compressed while crossing the pubic bone.
Summary
Thus, weakness and pain in the legs, with or without swelling, may indicate vascular compression syndromes. These conditions can directly affect venous drainage from the legs by compressing the femoral vein at the pubic bone and the popliteal vein at the tibial plateau and the femoral epicondyle. This can result in an inability to walk long distances due to increasing pain and weakness caused by reduced muscle oxygenation.
However, weakness that is prominent even without physical exertion suggests spinal congestion as a result of collateral circulation from a compressed left renal vein via a tronc réno-rachidièn, or from a compressed left common iliac vein via the ascending lumbar vein and other collaterals flooding the spinal canal.