Here , I describe for the first time an important mechanism , the nephroptotic perfusion rearrangement, which much contributes to the enormous suffering from vascular compression syndromes, especially in patients with connective-tissue disorders.
This mechanism of rearranged renal volume perfusion is nowhere else described (to the best of my knowledge) and was detected during painstaking renal perfusion measurements in horizontal and vertical body postures in patients with vascular compression syndromes. I see regularly patients with severe vascular compression syndromes and perform examinations of all relevant blood vessels in different body postures. It is well known that many patients suffer more in certain body postures.
Only the functional colour Doppler ultrasound with PixelFlux perfusion measurements can find out the very reason of these enigmatic symptoms.
Since we (Dr. Jakob Scholbach (mathematician) and Prof. Thomas Scholbach (physician)) developed the PixelFlux method I was able to monitor the renal perfusion in 100 of patients in different body postures.
The meticulous examination technique is able to describe qualitatively and precisely the effect of gravitation onto the perfusion of many organs, including the kidneys.
I was able to see a tremendous reduction of the renal blood flow in patients with nephroptosis.
The nephroptotic perfusion rearrangement
Nephroptosis is a medical condition where the kidneys sink down as soon as the patient assumes a vertical body posture. This condition is known for decades but its influence onto the blood flow towards the kidneys remained undetected until the event of the PixelFlux technique.
Below I give an example of the changing blood flow in a patient with nephroptosis, more on the right side than on the left side:

In this patient the perfusion of the left kidney is reduced compared to the right one in the horizontal, lying position. This is due to a lordogenetic compression of the left renal vein (nutcracker syndrome). When the patient stands, the perfusion of the left kidney increases whereas the perfusion of the right kidney drops significantly.
After assuming an upright position the perfusion in the right kidney in general dropped remarkably by 77% (0.69÷3.01 = 0.23). The perfusion of the left kidney also dropped but to a much lesser extent: By only 12% (1.37÷1.56 = 0.88).
Moreover, the pressure sensitive subcapsular vessels in the distal cortex show an acute pressurisation of the renal parenchyma of the right kidney. This can be demonstrated by the profoundly decreasing subcapsular distal cortical perfusion compared to the perfusion of the proximal cortex.
This ratio is in a horizontal position on the right side 2.20÷3.41 = 0.65, and on the left side 0.93÷2.25 = 0.41. While standing it is on the right side 0.10 ÷ 1.34= 0.07, on the left-sided is 0.3 9÷2.73= 0.14. This ratio describes the pressure inside the renal parenchyma due to the swelling of the kidney, here because of congestion. The lower the ratio is , the higher the pressure onto the tiny subcapsular vessels in the distal cortex. This ratio thus indicates very sensitively haemodynamic problems due to congestion or other causes of swelling of the kidney.
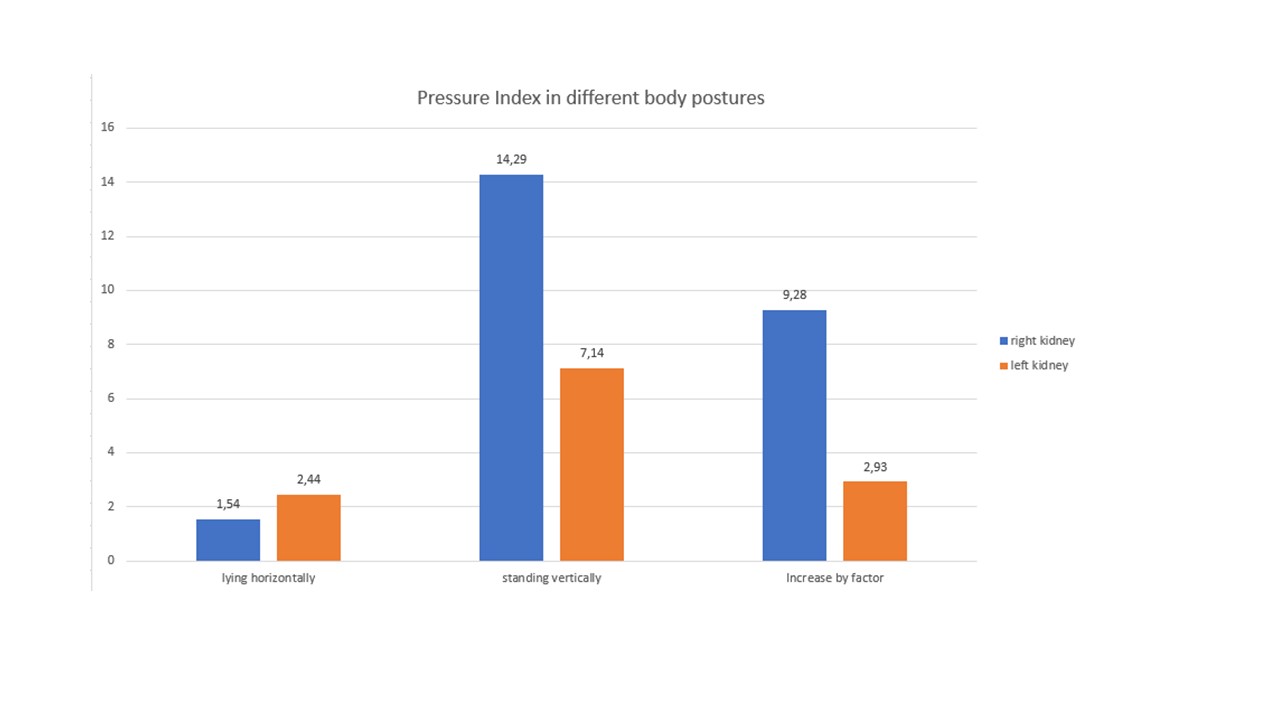
The PixelFlux-pressure index
The reciprokal ratio thus can be read as the degree of the venous congestion in acute situations, as a pressure index. This pressure index was in a lying position on the right side 1.54 and on the left side 2.44. This changed while assuming a standing posture: On the right side it increased dramatically to 14.29 and on the left side to 7.14.
This can be translated to pathophysiology as follows:
The left kidney has a chronic outflow obstruction because of the compression of the left renal vein in both body postures. That is why the right kidney accepts blood which normally would run into the left kidney. The volume load right/left in a supine position is 3.01÷1.56= 1.93, while standing it is 0.69÷1.37= 0.50.
The strong ptosis of the right kidney strangulates its blood flow by 77%.
The left kidney tries to take over but cannot let pass this sudden excess supply. The kidney also sinks down, albeit in a lesser extent and thus also reduces its perfusion by 12%. So, the already diminished perfusion of the left kidney suffers further while the patient is standing upright and cannot take over the amount which now cannot pass the right kidney anymore because of the stronger stretching of its blood vessels. That is why the patient experiences much more severe symptoms while standing upright and has to lie down frequently.
The nephroptotic stretch model
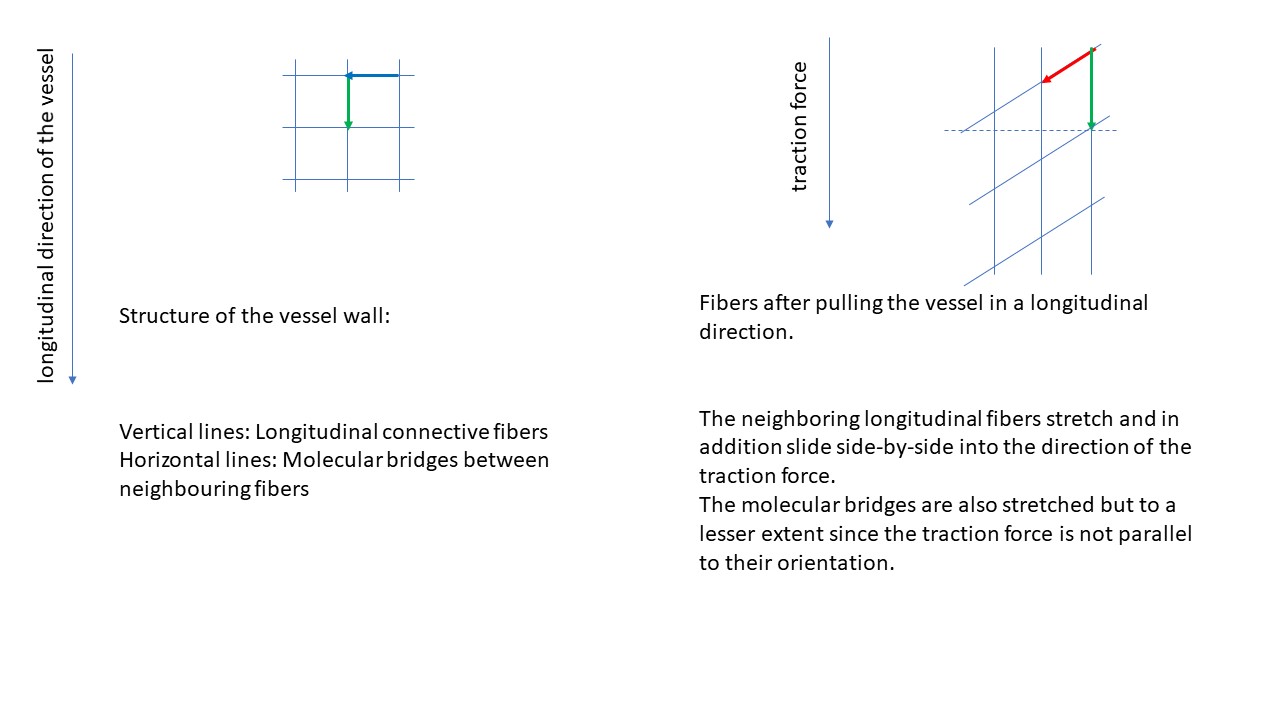
Stretching of a blood vessel
When a blood vessel is stretched the material of the wall has to be distributed onto the new shape of the vessel. The vessel can be perceived as a surface surrounding a cylinder. During stretching the material of the vessel wall has to be relocated. Some of the material is moved towards locations which are primarily outside the unstretched vessel. This can only be achieved by reducing the wall thickness and by narrowing the vessel.
The principle is outlined in the picture below:

Mathematical considerations for longitudinal traction on a blood vessel
Originally, the vessel consists of a certain amount of tissue which is used to build up the vessel wall. During stretching of the vessel by traction in the longitudinal direction the amount of tissue does not change. Nevertheless, the length of the vessel changes. Since the mass of tissue of the vessel wall can be described by the diameter of the vessel, its length and its wall thickness, these parameters must adjust, when one of them changes.
The tissue volume of a certain vessel segment can be described as follows:
V = 2 * ∏ * r * l * t
V – Volume of the wall tissue
r – radius of the vessel
l – length of the vessel segment
t – thickness of the vessel wall
When the vessel is pulled in a longitudinal direction, the length of the vessel segment under observation increases. Since the volume of the wall-segment must remain constant, the radius and the thickness of the wall must decrease. The extent of the reduction of radius and thickness depend on the mechanical properties of the wall tissue. The following table and diagram describe the relationship of vessel length and vessel radius under the assumption that the thickness of the wall remains constant. If it is assumed, that the wall thickness diminishes as well, the reduction of the diameter will be less then if we assume, that the wall thickness remains constant. Nevertheless, the formula describes the principal changes and their roughly expected degree to give an idea of postural changes in patients with nephroptosis.

How does nephroptosis affect symptoms and the distribution of blood between both kidneys?
Usually, the right kidney is more affected by gravity than the left one. This is due to the weight of the liver which forces the right kidney to sink deeper, since the smaller spleen has a less effect onto the left kidney. That is why the right renal vein and artery are more stretched than the left ones. Thus, the diameter reduction of the renal vessels on the right side is stronger than on the left side. The blood flow is distributed towards both kidneys evenly if no obstacle for the blood flow exists. The equal driving force for the blood flow towards both kidneys is the blood pressure. The blood pressure may change after transition from the horizontal to the vertical body posture, but it is nevertheless the same for both kidneys in vertical as well as horizontal position. Thus, the stronger stretching of the right renal vessels produce a significant reduction of the blood flow volume towards the right kidney. That is why the left kidney has to accept a proportional increase of blood volume.
In patients with a higher distensibility of connective-tissue (connective-tissue disorders e.g., Ehlers-Danlos syndrome) the stretching will be remarkably stronger than in healthy patients. Since patients with connective-tissue disorders are prone to vascular compressions they very often suffer from a left renal vein compression. Thus , the sudden increase of blood volume running into the left kidney in ptosis of the right kidney will cause a further increase of intrarenal pressure and the pressure of the collateral pathways of the congested left renal vein. This very often produces a severe increase of their symptoms, for instance in the skull, in the spinal canal , in the genitals and pelvic region as well as in the left flank.