- Новые статьи
- Частная рактика для функциональной ультразвуковой диагностики для детей и взрослых
- Сосудистые явления сжатия
- Лечение сосудистых компрессионных синдромов
- Недавно открытые синдромы сдавления сосудов
- Калейдоскоп поучительных дел
- Ультразвуковая диагностика
- Услуги
- Функциональный цветной допплеровский ультразвук — как я это делаю
- Иссле́дование
- Квалификация
- Вирус болезни Борна (ВББ) или Борнавирус
- Научное сотрудничество
- Cookie Policy
- Cookie Policy (EU)
A full urinary bladder and the internal iliac artery squeeze the external iliac vein on the right side, causing a new compression syndrome.
A 24-year-old male patient presented with increasing pelvic pain, a left-sided varicocele and erectile dysfunction. After ligation of the left spermatic vein to treat the varicocele, the symptoms were indicative of May–Thurner syndrome. Two overlapping stents were subsequently inserted into the left common iliac vein and the left external iliac vein to prevent compression of the left common iliac vein by the overriding right common iliac artery, which is characteristic of May–Thurner syndrome.
Following this intervention in 2023, the patient experienced only partial relief from the pelvic pain and erectile dysfunction. However, he still experienced unbearable pain when sitting for long periods, which prevented him from working. He also now complains of severe burning pain in his right upper thigh, especially after night-time rest, which is substantially alleviated by post-nocturnal micturition and walking around. He continues to experience burning and cramping pain in both his buttocks and upper thighs, as well as in his left flank.
A colour Doppler sonographic examination revealed patent stents in the left external and common iliac veins. However, the cranial end of the common iliac venous stent was significantly compressed in the sagittal plane (12–3 mm). However, the flow velocity was not accelerated, indicating the haemodynamic irrelevance of this partial compression of the stent.
About 5 cm cranial to the confluence of the two common iliac veins, a turbulent flow acceleration was detected within the vena cava, which, however, did not cause significant flow acceleration. Compression of the vena cava had developed due to exaggerated lumbar lordosis in the obese patient.
Within the right external iliac vein, a localised narrowing of the vessel with significant flow acceleration was demonstrated 1.5 cm caudal to the confluence with the internal iliac vein while the urinary bladder was full.

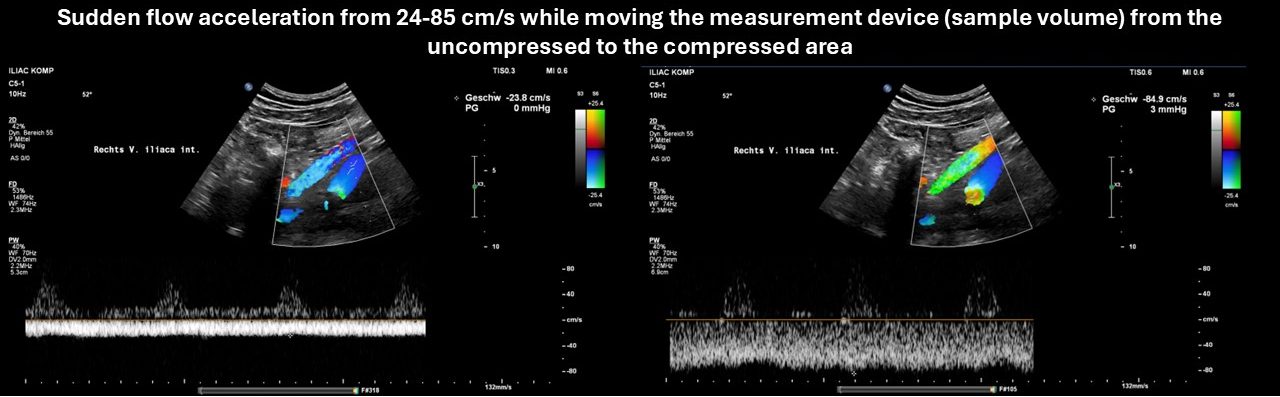



After micturition, the narrowing of the vein and the flow acceleration disappeared, reappearing after the bladder was subsequently filled following the oral intake of water.



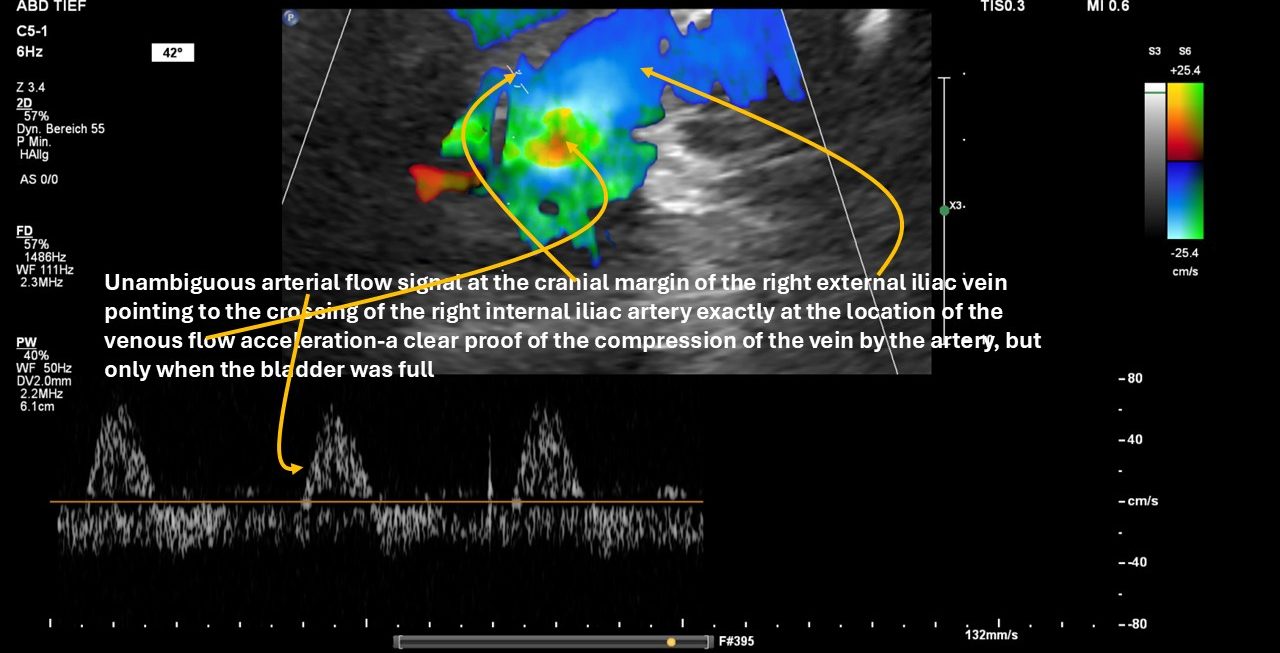
The variable compression of the right external iliac vein was due to the respective area being pinched between the obliquely crossing right internal iliac artery and the cranial part of the full bladder.
Thus, this variable vascular compression syndrome, which had not been described before, conclusively explained the post-nocturnal pain in the upper thigh, which disappeared after morning micturition.
This observation highlights the importance of performing a functional colour Doppler sonographic examination with flow quantification in circumstances that trigger the patient’s symptoms — in this case, a full urinary bladder.
Increasing pressure from a filling bladder produced an outflow obstruction in the right leg, responsible for the variable burning pain in the upper thigh.